Addressing Workplace Violence in Health Care Settings

Violence in health care is on the rise, jeopardizing the safety and well-being of employees as well as patient care. Standardized violence measurement tools can help workplaces anticipate and ultimately mitigate violent incidents. Read one medical professional’s personal experiences and recommendations for better action planning and listen to the full on-demand webinar to earn one contact hour.
The following includes summaries of actual incidents. Details have been changed to maintain the confidentiality of all involved parties.
Workplace violence is on the rise across sectors. However, health care and social service workers are five times more likely to experience workplace violence and suffer resulting physical and/or psychological trauma than employees in any other U.S. field.
Between 2011 and 2018, the incidence rate of non-fatal workplace violence inflicted upon healthcare workers nearly doubled, rising from a little over six incidents per 10,000 full-time workers to more than ten. Nearly 75 percent of critical care workers say they have experienced violence in the past year. And it’s important to note that health care violence isn’t inflicted on employees exclusively. It can occur between and among coworkers, patients, and patients’ families and guests. As of 2023, bedside nurses have the highest susceptibility to physical or even sexual abuse compared to other roles within health care.
Put another way, there’s no shortage of data proving that this is a problem, and a mounting one. Pending legislation including the Workplace Violence Prevention for Health Care and Social Service Workers Act aims to address health care violence at the federal level – a step in the right direction. In the meantime, it is the responsibility of health care organizations to comprehensively and effectively address this complex matter.
Luckily, a number of reliable and proven frameworks exist for mitigating health care violence. Keep in mind, though: to be effective, initiatives must reflect the exact drivers and scenarios that are present within any given workplace, which can vary dramatically. This requires examination of causation before initiatives can be launched. We’ll offer options for extracting causation below. But first, I’d like to share some personal experiences that compelled me to invest in this topic professionally as well as personally.
TWO JARRING HEALTH CARE OBSERVATIONS
Throughout my career, I’ve helped health care settings develop well-considered programs designed to sustainably and effectively address matters ranging from safe patient handling and mobility (SPHM) to caregiver injury prevention. These topics can brush up against workplace violence; however, it was two specific and unsettling experiences that compelled me to look more closely at rising workplace violence in health care settings:
- Several years ago, I was investigating an incident where a nurse had her right hand grabbed by a patient to whom she was providing care. He’d twisted it severely, resulting in significant injury to her dominant thumb and wrist. When I asked the nurse how she had responded in the moment, her answer was to the effect of, the customer is always right. That she should have been more careful. That her role is to serve her patients, even if it means jeopardizing her own safety to ensure care. It was an aha moment for me. How, I wondered, do we empower staff to not only protect themselves but to recognize that they should not tolerate this behavior? Healthcare is full of compassionate professionals who can succumb to this line of thinking. It’s all the more reason for organizations to equip them to understand and appreciate their own rights related to workplace violence, and to give them the tools they need and deserve.
- The second incident was one of the worst caregiver injuries I’ve been involved in investigating. A nurse in a multi-specialty unit was using a sling to move a patient from a bed to a chair when the patient grabbed the hanger bar – the bar the sling is attached to – and struck the nurse on the head multiple times, resulting in significant physical injuries and trauma.
Combined with other scenarios I’d observed or heard about anecdotally, these incidents raised my awareness of, and frustration with, the impact violence was having on personnel and the lack of an actionable assessment or screening tools to help anticipate potential for violence. This compelled me to look more closely at how workplace violence incidents are investigated and coded, with the hopes of driving better action planning and future prevention. Then and now, my stance on the matter tends to align with a quote from Erin Jaynes, MSN, RN, and former CNE:
“To fully address the growing issue of workplace violence, it’s essential that healthcare organizations today provide their staff with comprehensive solutions, tools, and processes necessary to prevent and respond to workplace violence.”
Fortuitously, my own aha moments occurred around the same time the Occupational Safety and Health Administration (OSHA) was prioritizing the matter of workplace violence.
OSHA AND INFORMATION GATHERING TOOLS
In 2016, OSHA began its formal push for awareness of, commitment to, and standardization of workplace violence prevention in health care. Their Guidelines for Preventing Workplace Violence for Healthcare and Social Services Workers offers recommended analysis and hazard identification, prevention and control, safety and health training, and record keeping and program evaluation. Many healthcare settings took these recommendations to heart in 2016 and in the years following. However, as is often the case with workplace initiatives, not all have maintained fervor since. It raises the question I implore all workplace professionals to ask themselves: Has your workplace built a sustainable and effective program? Have you implemented all of the things that you can to mitigate and manage workplace violence to the best of your ability? It is one thing, after all, to review data and track events. It’s another altogether to implement and standardize tools, solutions, preventions, and precautions that are going to have a significant impact on frontline workers.
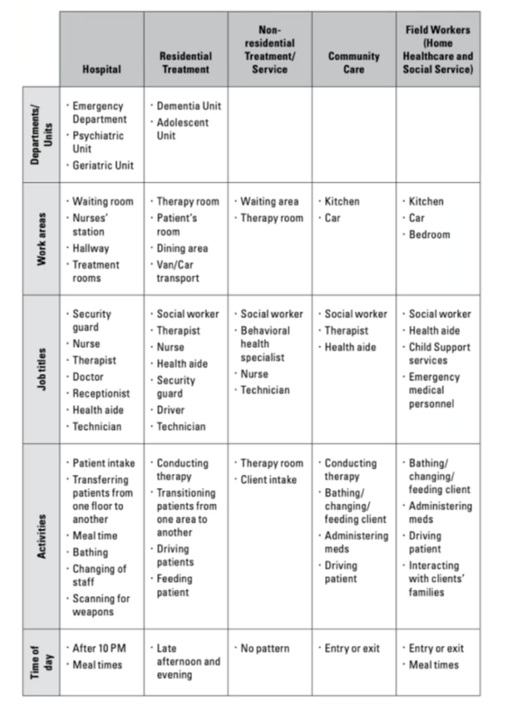
If the answer is no, a great place to start is with data collection designed to determine underlying causes – essential to coming up with solutions. Mental illness, drugs, and alcohol contribute to a large percentage of health care violence incidents; however, there are many other possible causes, and no two settings are the same. OSHA tools including this checklist that can help organizations pinpoint causation, patterns, and problem spots:
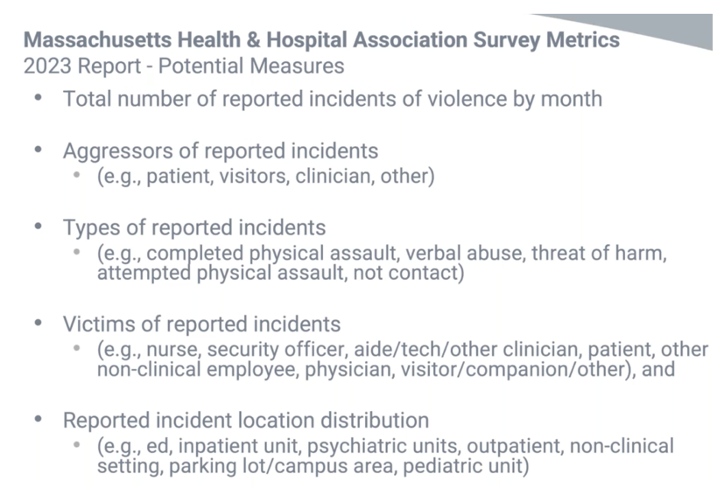
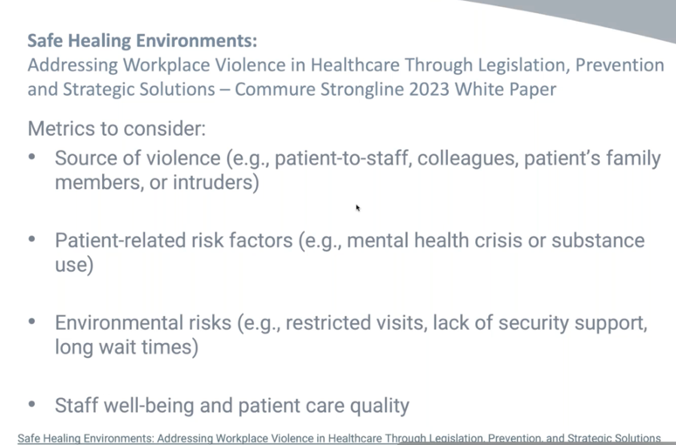
Several more frameworks also exist to assist in information gathering, including the Massachusetts Health & Hospital Association survey metrics and a white paper published by Commure, manufacturers of Strongline Pro alert technology:
TOOLS FOR INVESTIGATION AND RELATED DOCUMENTATION
Consistent and comprehensive injury investigation documentation is another key to tracking toward effective workplace violence initiatives. One readily available tool is the National Correct Coding Initiative (NCCI) coding system. Developed by the Centers for Medicare & Medicaid Services (CMS) to promote accurate medical coding, this system is not necessarily designed for tracking and trending patterns among violent incidents; however, it can be used that way – especially with a few modifications for internal use.
In the NCCI framework, code 74 indicates that an employee has been struck or injured by a fellow employee or patient. However, it does not offer the opportunity to specify whether the incident was accidental or deliberate, and whether it was an employee or patient who inflicted it. Wanting to use this coding system to help differentiate between these scenarios for tracking purposes, I added – again, for internal use only – subcodes 74a, 74b, and 74o beneath major code 74:
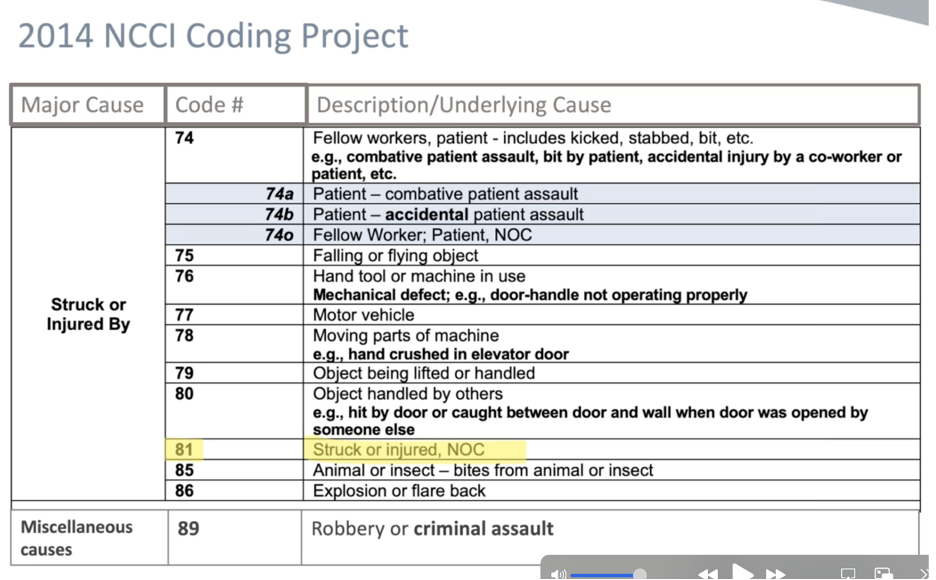
If using NCCI Codes in your workplace, please also note code 81 can mar information gathering related to violence. Code 81 reads, “Struck or injured, NOC.” NOC stands for no other cause. Be sure not to use code 81 for violent incidents. A better-fit code might be the aforementioned code 74 or maybe even code 89: which includes criminal assault.
AGGRESSION ASSESSMENT TOOLS
The Centers for Disease Control and Prevention (CDC) encourages health care settings to evaluate a patient’s observable status relative to aggression, and mentions the following tools: the Triage Tool (a series of questions based on research with abused women), the STAMP (focused on staring and eye contact, tone and volume of voice, anxiety, mumbling, pacing), and the Assault and Homicidal Danger Assessment Tool. A number of hospitals I’ve worked with either use or are actively exploring qualified tools. They’ve indicated that they want an aggression equivalent of the BMAT – the Bedside Mobility Assessment Tool. In other words, a tool that looks at a patient’s current status, real-time situation, and other relevant factors, then clues healthcare workers into the likelihood of aggression. One of the leading tools on this front that meets the criteria for real-time/current status is:
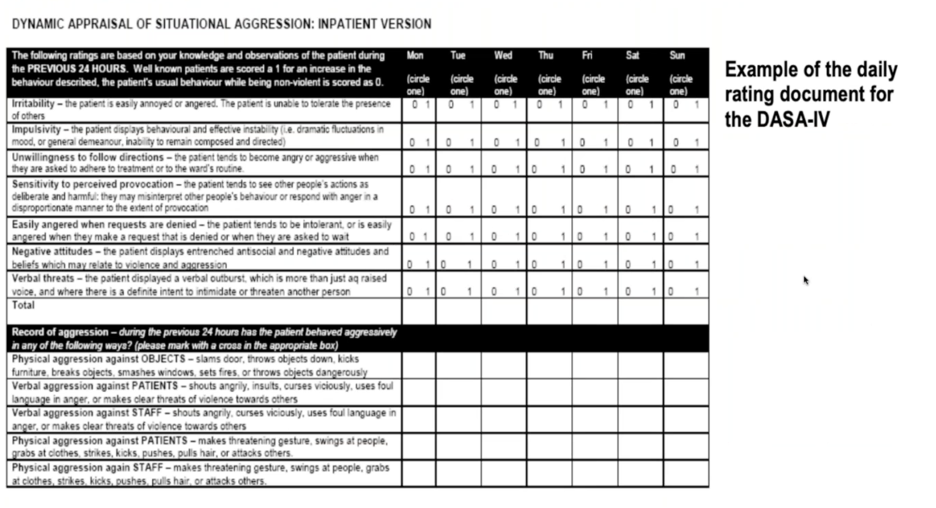
- The Dynamic Appraisal of Situational Aggression (DASA). The resource I see utilized most, DASA is a risk assessment tool designed not only to appraise a patient’s likelihood of violence, but to prevent communication breakdowns that sometimes occur when shifts change, or among health care workers in general. DASA asks a main nurse to complete a series of questions at least once a day, ideally soon after a patient is admitted (when aggression is most likely to present) and/or close to the time of a shift change or patient handover. Scoring indicates a patient’s likelihood for aggression. Even more, it indicates whether or not remedial action or monitoring is recommended. While DASA serves many purposes, I particularly appreciate its focus on alerting incoming staff of a patient’s recent behavior, which can go a long way toward keeping personnel safe.
There is no simple solution to ending workplace violence. Effective solutions require an ongoing, proactive, and multifaceted approach. This is worthwhile for all reasons, including the inherent right of health care professionals to have the tools and support needed to protect themselves in the event of workplace violence. After all, in any professional climate, but especially amidst ongoing nursing shortages, it’s tragic when a professional caregiver has to leave their chosen profession, temporarily or permanently, due to a life-altering, violence-inflicted injury. The mental, emotional, psychological impact can be similarly catastrophic, with long-term consequences
Of course, this is just the tip of the iceberg. Learn more about workplace violence prevention and mitigation initiatives and earn one free contact hour by listening to the full on-demand webinar.
Teresa Boynton, MS, OTR, CSPHP

Currently an independent consultant, from 2015 to 2018 Teresa Boynton, MS, OTR, CSPHP worked for Hill-Rom, assisting healthcare facilities in building safe patient handling and mobility (SPMH) programs. Prior, Teresa worked for Banner Health for 26+ years where she focused on preventing caregiver injuries, resolving workers’ compensation claims, and implementing a standardized SPHM and fall prevention program. In 2003 she began work on what became the Bedside Mobility Assessment Tool (BMAT). She and nurse colleagues developed BMAT 2.0 and published an article and support tools in the July 2020 issue of American Nurse Journal. Teresa received a 2020 Innovation Award from the National Board for Certification in Occupational Therapy for her work on developing and implementing BMAT and related SPHM programs. She is a longtime member of the Association of Safe Patient Handling Professionals (ASPHP). In 2000, Teresa took a sabbatical and worked as a paralegal for a medical malpractice defense attorney where she gained a greater appreciation for standardized practice and accurate documentation – an experience that informs and energizes her work to this day.