Beyond Blood Sugar: Navigating Skin Complications in Diabetes

Skin complications are more common in patients with diabetes than in the general population. Even more, they’re often more severe, pointing to the critical importance of early recognition and intervention. Below, gain insights on identifying pathology for a wide range of skin complications and learn about risk factors, prevention, and treatment relative to this uniquely vulnerable population. Listen to the full on-demand webinar to earn one contact hour.
Discussion of diabetes tends to focus on blood sugar, kidneys, and vision. However, another anatomical feature warrants a place in the conversation: Skin.
The body’s largest organ, skin is one of most common places where diabetes leaves its mark. Approximately 70% of people with diabetes will experience a skin disorder in their lifetime.1 Beyond frequency, the larger concern is risk. Skin complications are particularly high stakes in diabetics, adding urgency to all aspects of care. It’s imperative that care providers understand diabetes’ overall impact on skin and its role in specific skin conditions – which sometimes look different in patients with diabetes than in the general population.
THE IMPACT OF DIABETES ON SKIN
Understanding skin complications in patients with diabetes starts by understanding causation: Why are patients with diabetes at greater risk?
Long-term hyperglycemia, or chronically high blood sugar, is the common denominator. Prevalent when diabetes is not well-controlled, long-term hyperglycemia has widespread effects for skin including:
- Microvascular damage. When blood sugar stays high for prolonged periods, it sticks to proteins in blood vessels, creating a harmful substance known as advanced glycation end-products, or AGEs. AGEs stiffen blood vessels, decreasing blood flow. Over time, poor circulation results in slowed healing and higher risk of infection. Microvascular damage tends to be most severe in lower extremities.
- Neuropathy. When high levels of glucose enter the bloodstream, peripheral nerves – specifically, their tiny unmyelinated nerve fibers – are damaged, causing what’s known as diabetic neuropathy. Effects on skin include sensation loss, which can hinder skin injury symptom recognition, increasing chances of progression to ulcers and infection.
- Impaired immune function. Normally, white blood cells move quickly towards infection. But when blood sugar is high – hyperglycemia – chemotaxis, phagocytosis, and microbial killing are inhibited.
- Altered collagen and extracellular matrix. Glucose-mediated cross-linking of collagen alters tissue, including its structure and elasticity. For many individuals with diabetes, this means reduced skin integrity including stiff skin and poor wound healing.
- Inflammatory response. Hyperglycemia promotes a pro-inflammatory state that can contribute to dermal inflammation and fibrosis and can facilitate infection, worsening chronic wounds.
Understanding the larger relationship between diabetes and skin, let’s move on to related and resulting skin complications. Note that these conditions are not exclusive to patients with diabetes; however, they’re more common and high risk, requiring added vigilance and consideration.
SKIN INFECTIONS
Let’s break this down into three types of skin infections – bacterial, fungal, and viral. First, we’ll review bacterial infections.

Staphylococcus aureus and Streptococcus species are the most common bacterial pathogens. Symptoms typically include redness, warmth, swelling, and purulent discharge. Diagnosis comes via clinical evaluation and cultures gauging antibiotic resistance. Below are four bacterial infections more prevalent in diabetics than in the general population:

- Erysipelas and cellulitis. These bacterial infections cause redness, swelling, pain, and sometimes fever.Of the two, erysipelas – at left –is the more superficial and better demarcated. Cellulitis, at right, is red, hot, angular, and not demarcated – indicative of deeper infection. Both are treated with antibiotics – oral or IV, at the provider’s discretion.

- Necrotizing fasciitis. Rare but life-threatening, necrotizing fasciitis (sometimes called flesh-eating disease) presents as erythema and progresses quickly to blistering and hemorrhagic bullae, or blood-filled blisters. Most common in lower extremities, necrotizing fasciitis has a 20% mortality rate and puts patients at high risk of sepsis; suspected cases therefore must be treated emergently.2 Treatment typically includes surgery and/or a broad spectrum of antibiotics.

- Malignant otitis externa. An invasive bacterial infection of the outer ear, malignant otitis externa is rare but life-threatening, with a 10% to 20% mortality rate.3 It can spread rapidly, progressing to osteomyelitis and spondylitis and potentially leading to meningitis. Typically caused by pseudomonas, symptoms include severe ear pain and discharge. There’s not always a predetermining factor; however, this infection sometimes goes hand in hand with headphone use that can introduce pseudomonas into the ear canal. Treatment might include systemic antibiotics, surgery on the mastoid bone, and hyperbaric oxygen.
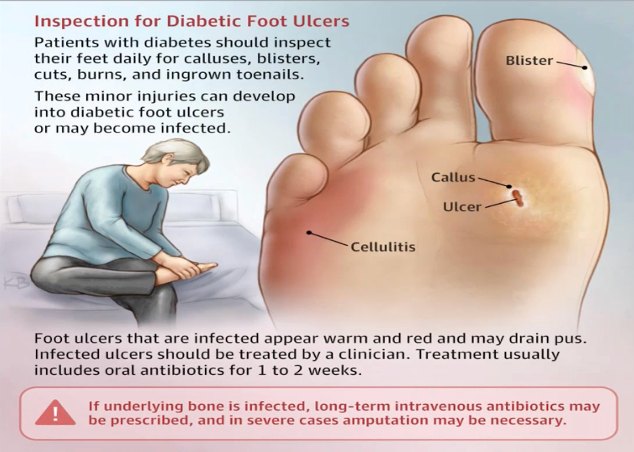
- Diabetic foot infection. Individuals with diabetes are prone to foot infection, and specifically, soft tissue infection – often staph or pseudomonal but sometimes can be polymicrobial, i.e., caused by two or more microorganism types. Given heightened risk of amputation among diabetic patients, it’s essential that feet are inspected daily for calluses, blisters, cuts, burns, and ingrown toenails or toenail infections that could become infected or develop into ulcers. The American Medical Association image above shows patients how to inspect feet. If a patient cannot inspect their own feet, it’s essential that someone else does it for them. Remember that calluses, blisters, cuts, and burns can be interdigital. Treatment for diabetic foot infection ranges from topical to oral antibiotics to surgical debridement. It almost always requires multidisciplinary care across podiatry, endocrinology, and orthopedic teams.
Fungal infections feed off sugar, hence their prevalence in patients experiencing hyperglycemia. Several fungal pathogens exist in addition to general fungal infections, which are characterized by itching, redness, scaling, and fissures. All are diagnosed via a fungal culture. The four most common processes seen among diabetic patients are:
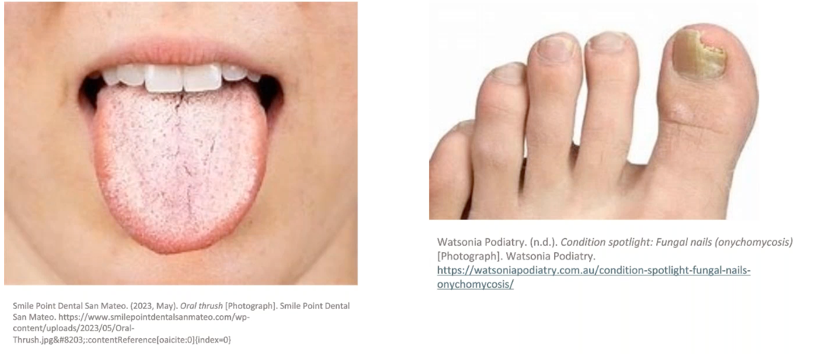
- Candidiasis, or Candida. Thriving on sugar, Candidiasisis another early marker of high blood sugar complications. If a patient without a formal diabetes diagnosis has recurrent Candidiasis, and especially if there’s no family history of Candida or eating disorders (which can increase oral Candida carriage)4, diabetes testing is recommended. Pathology behind Candidiasis is elevated salivary glucose and skin pH that support the growth of fungi caused by an overgrowth of the Candida species of yeast. Thrush on the tongue and thick, discolored toenails are common symptoms. Treatment for Candida is anti-fungal therapy, either topical or oral, at the discretion of a provider. Glucose control is also key.

- Dermatophytes. Tinea infections and dermatophytosis are often used interchangeably; both refer to fungal skin infections caused by dermatophytes. These infections present as itchy and painful periodic, bullous lesions. The key concern in diabetic patients is the risk of secondary infection. Patients often scratch at tinea infections, resulting in, or exacerbating, open skin. Individuals with tinea infections often have diabetic neuropathy that diminishes sensation, making them unlikely to feel the onset of any infection, exacerbating risk. Treatment is most often topical. Types of tinea infections, including their common names, include:
| Type | Common Name | Location | Key Features |
|---|---|---|---|
| Tinea Corporis | Ringworm | Arms, legs, trunk | Circular, red, scaly pathes with clear center |
| Tinea Pedis | Athlete’s | Feet, between toes | Itching, peeling, cracking skin |
| Tinea Cruris | Jock Itch | Groin, inner thighs, buttocks | Red, itchy rash, often ring-shaped |
| Tinea Capitits | Scalp Ringworm | Scalp, hair | Hair loss, scaly patches, “black dots” |
| Tinea Unguium | Nail Fungus | Toenails, fingernails | Thickened, discolored, brittle nails |
| Tinea Barbae | Beard Fungus | Beard, neck, face | Red, swollen patches, sometimes pustules |
| Tinea Faciei | Facial Ringworm | Face (excluding beard area) | Red, scaly patches, can mimic other conditions |
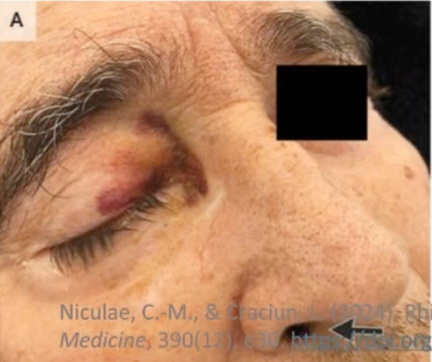
- Mucormycosis. Rare but aggressive, Mucormycosis thrives in areas with hyperglycemia and in acidic environments. Patients with Type 1 diabetes are at greatest risk, especially if they have diabetic ketoacidosis (DKA). Mucormycosis’s presentation is typically rhino-orbital, cerebral, with sinusitis, headache, facial edema, and tissue necrosis – the last of which introduces the greatest urgency and risk. Tissue necrosis warrants early intervention, usually consisting of surgical debridement and IV amplification.
Like bacterial and fungal infections, viral skin infections are seen more often in patients with diabetes than in the general population. They typically present as painful blistering and burning sensations, often near a dermatome (areas of skin that connect to a nerve root on the spine). Viral skin infections are diagnosed via PCR viral culture testing. Treatment is case-dependent. Here are four viral infections seen most often in patients with diabetes:

- HPV. Short for Human Papillomavirus, HPV is extremely common, affecting 80% of sexually active adults at some point in their lives.5 It occurs when the HPV virus affects epithelial cells, causing hyperproliferation which forms warts that present most often on feet, at the nape of the neck, at pressure points, or on fingers. Because of immune dysfunction, individuals with diabetes generally experience HPV more severely than the general population and are prone to more severe skin breakdown around warts, as well as related risks such as bacterial infection. HPV can elude treatment; modalities are therefore vast, and include cryotherapy, topical agents, salicylic acid, and surgical removal. Treatment determination often requires involvement of specialists including dermatologists.
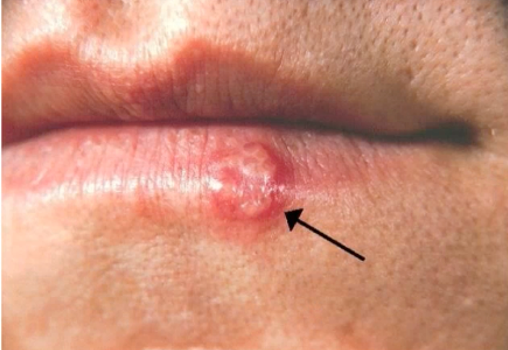
- Herpes simplex. Sometimes abbreviated HSV, Herpes simplex affects 67% of the general population under age 50.6 Presentation consists of small, fluid-filled blisters called vesicles atop a red erythematous base. After initial exposure, the virus stays latent in nerve ganglia, reactivating in times of stress, illness, or general immunosuppression. Due to immunosuppression, outbreaks in diabetic individuals tend to be more frequent and more prolonged, introducing risk including bacterial infection. A wide array of antivirals is available as treatment; these antivirals aim to shorten outbreaks and reduce occurrence frequency.

- Molluscum contagiosum. Caused by a virus of the same name, molluscum contagiosum is characterized by dome-shaped lesions, each with a central dimple or “button.” Molluscum contagiosum is common among immunocompromised individuals and therefore diabetics – another example of an infection that can be an early indication of diabetes, especially if a patient has no family history of the infection. Though they can present on any body surface, lesions appear most commonly on the axilla, lower portion of legs. Lesions can be resistant to treatment; they also introduce risk of bacterial infection. Common treatment includes cryotherapy, topical treatment, and, again, improving glycemic control.

- Herpes zoster. Commonly known as the shingles virus, Herpes zoster presents as a painful, unilateral, and vesicular rash; pain typically proceeds the rash’s appearance. It invariably follows a dermatome. Like Herpes simplex, Herpes zoster remains latent after initial exposure and can reemerge in any scenario, and especially amidst stress and immunosuppression. Postherpetic neuralgia (PHN) is common here, and uniquely painful. Antivirals, ideally administered within 72 hours of symptoms, are the ideal treatment; pain control is often also advisable.
DIABETIC FOOT ULCERS (DFUs) AND NEUROPATHIC ULCERS
There is a strong correlation between diabetic foot ulcers and amputation. There’s also a strong correlation between amputation and death, and other adverse outcomes – hence the importance of awareness and early intervention of DFUs and neuropathy in diabetic patients. A little more on the tenets of symptoms, diagnosis, treatment, and prevention:
Diabetic Foot Ulcer
| Symptoms and Diagnosis | Treatment and Prevention |
|---|---|
| Symptoms: Painless lesions, drainage, foul odor. Diagnosis: Clinical examination, wound assessment, ankle-brachial index (ABI) for circulation. | – Regular foot inspections and hygiene. – Wound care: Debridement, infection control, dressing selection. – Offloading pressure: Use of orthotics or special footwear. – Advanced treatments: Hyperbaric oxygen therapy, negative pressure wound therapy (NPWT). – Preventing recurrence: Blood sugar control, appropriate footwear, and patient education. |
PRESSURE INJURIES
Diabetics are also at increased risk of pressure injuries, for many reasons including the fact that they often struggle to feel and therefore miss early warning signs. Here are some tenets of pressure injury symptoms, diagnosis, prevention, and treatment:
| Symptoms and Diagnosis | Treatment and Prevention |
|---|---|
| Early signs: Reddening of the skin, localized swelling, skin breakdown. Diagnosis: Staging of pressure injuries based on depth (Stage I to IV). | – Preventative measures: Regular repositioning, pressure-relieving devices (mattresses, cushions). – Wound care: Moist wound healing principles, use of hydrocolloids, alginates, and foams. – Infection control: Topical and systemic antibiotics if healing is not progressing. |
OTHER SKIN CONDITIONS
Far less common than those above, these skin conditions nonetheless need to be understood by caregivers:

- Diabetic dermopothy. Often referred to as shin spots, symptoms of diabetic dermopathy – small, round, and brown-ish patches – present in 30 to 60% of diabetic patients, and most often in older adults with longstanding and/or poorly controlled diabetes. Sometimes they’re so subtle that you don’t notice them unless you’re looking for them. Diabetic dermopathy is linked to microvascular complications like those outlined earlier, which limit blood flow. Their telltale patches can also be induced by minor trauma, like bumping a leg. In terms of treatment: There is no treatment, as these go away on their own. Help them along by optimizing blood glucose control and protecting the area from external trauma.

- Acanthosis nigricans. Acanthosis nigricans is common in individuals with insulin resistance, and therefore in many adults with obesity and Type 2 diabetes. Occasionally, it is associated with malignancy and gastrointestinal cancers.
In terms of pathogenesis: excess insulin or insulin-like growth factors simulate keratinocyte and dermal fibroblast proliferation. Skin consequently gets thicker and more pigmented, appearing almost velvety. Acanthosis nigricans typically presents on the neck but is also seen in the axilla, the groin, and other skin folds.
Management and treatment focus on the underlying cause. If an individual is obese, weight loss can offset symptoms. If insulin resistance is at play, it is managed. For many diabetic patients, glycemic control is the focus.

- Skin tags. Skin tags are benign and extremely common, presenting in 50 to 60% of adults in the general population and most often in those with obesity, insulin resistance, and advancing age, as these factors promote epidermal proliferation.
Resulting from friction, skin tags are fleshy, hyper-pigmented growths appearing on the neck, axilla, groin, and sometimes the eyelids – areas where skin rubs against itself. Treatment is strictly cosmetic and ranges from surgical removal to cryotherapy.

- Bullous diabeticorum. An extremely rare blistering condition whose pathogenesis is unclear, bullous diabeticorum is most common in men with Type 1 diabetes. Age of onset is typically between 50 to 70 years old.
This condition goes hand in hand with diabetic complications like neuropathy, nephropathy, and retinopathy. Presentation is marked by sudden onset of blisters, most often in both bilateral lower extremities. Blisters heal in two to six weeks but frequently recur.
Possible causes for bullous diabeticorum are autoimmune factors, light exposure, neuropathy, and fluctuations in blood glucose. Preventing secondary infection is key here; blisters are usually left intact and monitored for signs of secondary symptoms.

- Necrobiosis lipoidica. Necrobiosis lipoidica is a rare, chronic, idiopathic skin condition most common in women with diabetes, and specifically Type 1 diabetes. In older adults, incidence among Type 2 diabetes increases.
Necrobiosis lipoidica presents as red-brown skin lesions that evolve to become waxy and yellow brown, as pictured. Lesions can ulcerate, requiring treatment to reduce risk of secondary infection. In terms of pathogenesis, the cause of necrobiosis lipoidica is unclear. This condition can evade treatment. Topical treatments, corticosteroid creams, and surgery are all options.
Want to learn more about skin complications relative to patients with diabetes? Earn one free contact hour by listening to the full on-demand webinar.
Elizabeth Doherty, MSN, CRNP, FNP-C

Elizabeth is a Family Nurse Practitioner with over 11 years of clinical experience. Her background includes emergency medicine, medical-surgical nursing, and pediatric emergency/urgent care. Elizabeth currently serves as a Clinical Education Specialist at HoverTech, where she combines her passion for safe patient handling and pressure injury prevention to support both nurses and the patients they care for. In addition to her role at HoverTech, she is an adjunct faculty member at DeSales University, where she enjoys educating and mentoring the next generation of nurses.