Happy Nurses and HAPI Prevention

Critically ill patients are uniquely susceptible to hospital acquired pressure injuries (often shortened to HAPIs), which create unhappy realities for patients, bedside care providers, and healthcare facilities. Below, discover nurse-driven strategies for the prevention of HAPIs in critical care and learn evidence-based techniques for safe patient handling and mobility. Listen to the full on-demand webinar to earn one contact hour.
There’s nothing happy about HAPIs, short for hospital-acquired pressure injuries – pressure injuries that develop during a patient’s stay at a hospital or facility. HAPIs cause patients significant discomfort and harm. They increase the risk of infection, related conditions, and complications including osteomyelitis. Pressure injuries including HAPIs have been associated with a 57% increased length of stay for patients, 5% increase in mortality, and 22% increase in 30-day readmission rates.1
These realities impact healthcare costs. Pressure injuries add more than $32,000 on average to ICU hospitalization costs. The total cost for severe cases generally ranges from $75,000 to $150,000 per pressure injury.2 Additionally, hospitals are required to notify the Centers for Medicare and Medicaid Services (CMS) when HAPIs develop in-house, which can result in reimbursement penalties.
Which brings us to HAPIs’ unhappy implications for bedside providers. Pressure injuries typically increase nursing care time and physical labor. And because HAPIs are nursing-sensitive indicators (NSIs), used to monitor care quality, they can also impact professional reputations.
These sobering statistics are true across patient populations but particularly distressing in critical care, which sees the highest prevalence of HAPIs compared to other acute care areas. Critical care patients are four times more likely to develop a severe HAPI during admission. The heightened vulnerability of critical care patients means HAPIs should be prevented at all costs. This, of course, is easier said than done.
The tools and strategies below are designed to help busy critical care nurses assess and prevent HAPI events. But first, a refresher on pressure injuries and a bit more on HAPIs in critical care specifically.
PRESSURE INJURY REFRESHER
According to the National Pressure Injury Advisory Panel, a pressure injury is localized damage to the skin and underlying soft tissue usually over a bony prominence or related to a medical or other device. The injury can be present as intact skin or an open ulcer and may be painful. The injury occurs as a result of intense and/or prolonged pressure or pressure in combination with shear. The tolerance of soft tissue for pressure and shear may also be affected by microclimate, nutrition, perfusion, co-morbidities and condition of the soft tissue.3
As seen above, the National Pressure Injury Advisory Panel’s definition of pressure injury is extensive, reflecting the complexity of this form of skin and soft tissue damage. Words in bold are highlighted for their unique implications for the critical care population.
Take medical devices. Critical care patients often require mechanical ventilation, NG tubes, central venous catheters, and cervical “C” collars, increasing the likelihood of pressure injuries given these devices’ frequent contact with skin.
Then there’s pressure in combination with shear. It’s widely understood that prolonged perpendicular force to the skin, called compression, can cause pressure injuries. However, the role of shearing and friction is often overlooked. In shearing, internal tissue moves against itself, generally at the bone-muscle interface. Friction can occur when skin moves against an object.Every nurse has boosted up a patient in bed…only to have them slide back down. That movement results in both friction and shearing, which play a more significant role in pressure injury development than is widely recognized. There are six distinct pressure injury stages. Deep tissue pressure injuries, considered a more severe pressure injury, have the highest prevalence rate of pressure injuries in the ICU, representing 33.6% of all critical care pressure injuries.
WHY CRITICAL CARE PATIENTS ARE SUSCEPTIBLE TO HAPIs
Some might assume that HAPIs in critical care stem from patient immobility. While immobility frequently contributes, it’s not the only cause. Medical literature reveals more than 100 risk factors for soft tissue injury. According to research by Cox and Schallom, these risk factors fall into three categories:
- Static intrinsic factors. Unchangeable baseline characteristics: age, immobility, history of smoking, peripheral artery disease, coronary artery disease, diabetes mellitus, end-stage renal disease.
- Dynamic intrinsic factors. Arising from critical illness, these can worsen or improve: hypotension, hypoxia, respiratory failure, anemia, hemodynamic instability, malnutrition.
- Dynamic extrinsic factors. These are external factors related to the treatment of critical illness: length of stay, OR time, vasopressors, mechanical ventilation, sedation, RRT, ECMO, devices.4
A 2022 study of more than 40,000 patients by Cox, et al. identified the top four contributors to pressure injuries among critically ill patients:
- Diabetes mellitus
- Mechanical ventilation
- Peripheral vascular disease
- Vasopressor agents
The practical conclusion is that impaired tissue oxygenation and perfusion are closely linked to pressure injury development in critical care settings.5
ASSESSING HAPI DEVELOPMENT IN CRITICAL CARE
HAPI assessment and HAPI prevention go hand in hand. However, assessment is only as good as the tools and scales used. Herein lies limitations. The Braden Scale – by far the most commonly-used assessment scale in the U.S. – comes up short in intensive care settings. It does not, for example, factor in degree of hypotension, vasopressor use, diabetes, and use of mechanical ventilation or other devices.
This puts the onus on healthcare systems and bedside providers to use precise assessment skills and develop standard practices for gauging pressure injury susceptibility and presentation. To do this effectively, providers must understand misconceptions that can get in the way of early recognition.
First, there’s the matter of skin color change. Color change and non-blanching are two ways to determine whether a pressure injury is brewing. However, these visible indicators are just a few of the signs.
Even more, the development of a deep tissue pressure injury precedes visible signs by about 48 hours. By the time a deep tissue injury is visually identifiable, it’s well underway. Here are some tools for effectively assessing those early signs of HAPI:
- Ensure skin is clean and moisturized. Beyond being good practice, using water to wet skin can help reveal subtle texture or color changes.
- Use halogen and natural light. Overhead lights, like fluorescent lights used in many healthcare settings, give off a blue hue. Whenever possible, use natural daylight and supplement with halogen or full-spectrum lighting for more accuracy.
- Palpate. Examine skin with fingers. Is it boggy? Soft? Firm? Does the patient have sensory changes? Pain? Are there temperature changes? For darkly pigmented skin, use the pads of four fingers.
- Compare affected vs. non-affected sites. Differences in temperature, texture, moisture, and feel from one spot to the next can be an indicator of pressure injury development. Assess temperature with the back of the hand to see if there’s coolness or heat. Skin that’s warmer than surrounding areas could indicate inflammation. Skin cooler than surrounding areas could indicate subpar perfusion.
ASSESSING PATIENTS WITH DARKER SKIN TONES
Added diligence among providers is needed for patients with darker skin tones. Blanching and skin color changes, such as erythema, often are not visibly apparent on darkly pigmented skin, on which tissue injury can present as gray, blue, darker pigmented, darker brown, black, or purple. When HAPI development is overlooked, it can have dire consequences. A few studies have shown a lower incidence of stage one pressure injuries, yet a higher incidence of more severe pressure injuries, in patients with darker skin. This likely indicates overlooked pressure injuries that often progress. Patients with darkly pigmented skin have also been reported to have higher mortality rates from pressure injuries, pointing yet again to the possibility of HAPIs going unnoticed, and health inequity overall.
A contributing factor here is the lack of diversity in skin tone photos in nursing education and literature. You’ve likely heard of the Fitzpatrick scale for skin tones. The Monk Skin Tone Scale, created by Harvard sociologist Dr. Ellis Monk, is more encompassing and diverse, and therefore recommended as the modern standard for assessing skin tones.
PREVENTION STRATEGIES
As bedside providers assess for pressure injuries, they also need to proactively prevent them – a tall order. Luckily, the National Pressure Injury Advisory Panel offers an evidence-based prevention checklist:
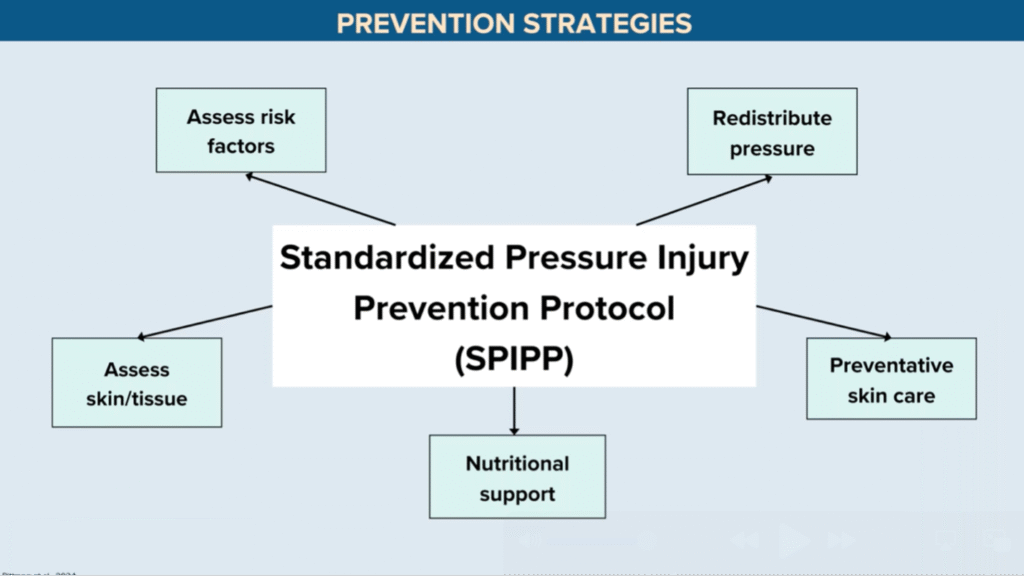
Let’s unpack each of these preventative measures, keeping in mind that to be effective, they must be:
- Implemented ASAP – ideally upon ICU admission
- Tailored to each patient
- Consistently applied across shifts and units
Redistribute pressure. At minimum, patients need to be repositioned every two to three hours, which can reduce the likelihood of HAPI development by as much as 14%. Beyond turning, pressure redistribution can include offloading high-risk areas (like heels), utilizing silicone multilayer foam dressing, and the utilization of wedges to maintain the 30-degree angle necessary to offload the susceptible sacrum and coccyx.
Preventative skincare. Preventative skincare applies to a number of scenarios. One is incontinence management. Indwelling catheters and other devices can help ensure that surrounding skin remains dry and free of moisture-associated skin damage. Weeping management is also key, as weeping is common in the ICU. Wicking material can aid in moisture management in these scenarios. Then there’s dryness prevention. Moisture can contribute to skin disruption, but so can overly dry skin. Utilize quality moisturizing agents to improve skin elasticity and prevent breakdown. Additionally, use as few layers as possible between a patient’s skin and the mattress – ideally less than three. This is essential to maintaining an optimal microclimate. Additional layers contribute to trapped heat and moisture, altering the microclimate and heightening HAPI risk.
Nutritional support. Nutritional support is essential for multiple reasons including its role in HAPI prevention. If patients develop pressure injuries, additional supplements can be incorporated to help facilitate wound healing.
Assess skin/tissue. As discussed, skin assessment is complex but vital. Some facilities practice the “two nurses, four eyes” protocol, in which two nurses conduct a thorough skin assessment, typically upon admission. If pressure injuries are present, document them in full. This includes taking photos that can be used as a baseline reference for skin assessment moving forward.
Assess risk. Patients should be evaluated for HAPI risk regularly, during every shift at minimum, and anytime there is a change in the patient’s clinical status overall. Risk assessment should include use of a validated screening tool such as the Braden Scale.
The evidence-based practices above are key to prevention but can be challenging in light of common barriers present in the healthcare system – lack of available nursing staff, for example, which one study found was the most common barrier for missed repositioning. Musculoskeletal pain and injury among providers is another, as is patient acuity. Critical care patients are, by definition, sicker than the general patient population. Patient acuity today is 3% higher than pre-pandemic levels.6 Sometimes a patient is simply too sick to turn – for example, some patients are too hemodynamically unstable to reposition given risk versus benefit.
HAPI SOLUTIONS IN PRACTICE
Luckily, there are numerous tactics and tools to help with HAPI prevention in practice:
- Verbal cues, dashboard alerts, and other reminders. 78.6% of respondents in one survey found these helpful for implementing HAPI prevention measures.
- Nursing rounds. Nursing rounds are shown to increase repositioning strategies by 30%.
- Turn teams. Turn teams can reduce pressure injuries from 15.1% to 5.2% – a significant drop.
- Pressure mapping technology. When two surfaces have various points of contact, pressure mapping technology can turn that data into color-coded images or a map highlighting areas’ respective pressure levels. This provides a visual cue of excessive pressure and guides repositioning.
- Wearable sensory devices. Worn by patients, these provide alerts for repositioning and can monitor the actual turn angle – namely, that 30-degree turn angle, which is essential to HAPI prevention.
- Nursing education. Crucial across the board, nursing education can introduce new tools and practices and keep key topics front of mind.
- Positioning systems. The data says it all: In one meta-analysis, implementation of a repositioning system reduced pressure injuries from 5.5% to 2%. Some of the possible components of an effective positioning system:
- Low-friction glide sheet with grip surface
- Handles to assist caregivers
- Built-in anti-shear strap
- Disposable microclimate body pad
- 30-degree body wedges
- Device training. Because musculoskeletal injuries are all too common in nursing, it’s essential to consider devices that not only help to mobilize patients but protect bedside caregivers as well. Some examples:
- Friction reducing sheets. Compared to manual handling with a standard bedsheet, friction reducing sheets minimize biomechanical loads for caregivers and risk of friction and shearing for patients.
- Air-assisted devices. These hook up to air and are placed underneath a patient, decreasing the biomechanical load needed for handling, turning, and transport. Compared to manual handling, air-assisted devices dramatically reduce risk of shearing and friction. Compared to standard draw sheets, they significantly reduce friction and biomechanical stress. Air-assisted devices also tend to be preferred by patients for comfort, ease, and integrity.
- Mechanical lifts – early mobility is key to improved health outcomes. However, ICU patients often require mobility assistance, and there is no such thing as “safe” manual patient lifting. You can employ the best body mechanics and still be at risk of injury. A solution is mechanical lifts, which offset biomechanical load. Employee injuries decreased by an astounding 73% in one study of manual lifting versus lifting via lift, with related cost avoidance of $171,600. When the option exists, ceiling lifts are preferable to floor lifts; however, floor lifts are still preferable to mechanical lifting.
HAPI ENDING
Fewer HAPIs mean happier nurses, happier organizations, and happier patients. Lean on the guidance above (suggestions for repositioning systems and mechanical lift use especially) to decrease HAPI events for happier outcomes. Eager to explore this topic further? Earn one free contact hour by listening to the full on-demand webinar.
Sarah Vance, MSN, RN, CCRN

With over 15 years of critical care experience, Sarah is dedicated to educating and mentoring nurses, both new and new to critical care. Sarah has a knack for simplifying complex concepts and bringing a lighthearted approach to the often intense ICU environment.
She shares valuable free open-access medical education content on social media, covering topics such as intra-aortic balloon pump placement, sedation and pain management for ventilated patients, and safe blood transfusion administration, all crucial for critical care nurses. She sees the nurse holistically, recognizing the emotional and interpersonal aspects in addition to the technical skills and protocols. She understands that nursing involves the heart, emotions, relationships, communication, and ongoing self-reflection.
- https://scholarlycommons.hcahealthcare.com/cgi/viewcontent.cgi?article=1922&context=hcahealthcarejournal
- https://www.sciencedirect.com/science/article/abs/pii/S0020748920300316
- https://cdn.ymaws.com/npiap.com/resource/resmgr/online_store/npiap_pressure_injury_stages.pdf
- https://pmc.ncbi.nlm.nih.gov/articles/PMC8776011/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC9200225/
- https://vizientinc-delivery.sitecorecontenthub.cloud/api/public/content/951ecf29635c466babe4d3efac23ce66