Less Sedation, More Mobility: Pursuit of an Awake and Walking ICU
Sedation is the default in most ICUs. Yet sedation is more detrimental to patient health than widely recognized for a variety of reasons including its hindrance to mobility. Below, hear Kali Dayton’s compelling case for sedating less frequently and more mindfully. Listen to the full on-demand webinar to earn one contact hour.
It’s a common ICU scene: a patient lying in bed, motionless, sedated. Among healthcare professionals and the public alike, this is generally believed to be the most comfortable and humane option for ICU patients, particularly those who are intubated. The perception is that they’re sleeping restfully and comfortably, free from pain.
In reality, sedation is far more complex and even harmful than meets the eye. Sedated patients are not sleeping. Propofol and opioids disrupt brain activity, making REM stages 3 and 4 impossible to achieve. Pain is not eradicated but rather distorted in a manner elaborated on below. Sedation has been linked to dire health outcomes we’ll also explore.
Beyond these drawbacks, sedation also goes hand in hand with atrophy. Sedation, after all, makes patients unable to move, resulting in a prolonged anti-gravity environment. Like astronauts returning to earth after extended periods, this leads to bone loss, muscle density and matter loss, cardiac deconditioning, insulin resistance, and orthostatic hypotension. Similarly, sedation prevents early mobility. Contrary to prevailing beliefs, early mobility is a safe and advisable intervention for most patients in the ICU, with fewer adverse events and more benefits than many realize, especially when compared to immobility.
In short, while often necessary and indicated, sedation does not need to be the default for ICU patients, including intubated patients. If this comes as a surprise to you, you’re not alone.
ARRIVING AT THIS OUTLOOK
My first experience in critical care came a few years into my nursing career, in 2012, at a high-acuity medical surgical ICU in Utah.
Walking intubated patients was central to the unit’s culture, was taught in my job training, and became a standard part of my shifts. Fellow nurses and I carefully but confidently awakened most patients immediately following intubation, gave them a clipboard for communicating, and began the process of getting them off restraints. Barring contraindication, most patients were, at minimum, sitting on the side of their bed within 12 hours. In many cases, they were walking within that same time window.
A few years later I moved on to a new position as a travel nurse in a different ICU in another state – and was perplexed. Why are our patients constantly sedated? I was told it was because they were intubated. This made no sense to me. I’d seen hundreds, if not thousands, of intubated patients awake and walking, I said – words that often fell on deaf ears or worse. The idea of mobilizing intubated patients, I was told by colleagues and even superiors, was inhumane, impossible, and ill-advised. Over time I came to realized that this second ICU setting was more representative of ICU norms.
Then, a few years ago, a woman with a familiar face approached me in public. “You were my nurse in the ICU,” she said. “You made me walk when I didn’t want to. I thought I hated you.”
It came flooding back: This woman had been a patient in the Utah ICU years prior. She’d written on her clipboard that she didn’t want to go to a nursing home. She wanted to be discharged home to her partner and her dog.
My fellow nurses and I knew she would not be extubated if her diaphragm weakened – which would prevent her from going directly home. And so, to preserve what diaphragm strength she had, we insisted she walk. This despite the fact that she was frail at baseline, with several comorbidities.
Suddenly this woman had me in a bear hug. “You saved my life,” she said.
My career since then has been dedicated to asking questions, researching, and ultimately advocating for what I call an awake and walking ICU, defined as follows:
- Sedation is given only when there’s an indication for sedation
- The safest sedative is given at the lowest dose for the shortest duration possible
- The highest level of mobility possible is performed unless there is a contraindication to mobility
- Open family visitation is encouraged and practiced
Consider this: Sedation hasn’t always been the norm. Through the 1980s, patients on mechanical ventilation were largely awake and often mobilized. This began to change in the 1990s. In efforts to offset acute respiratory distress syndrome (ARDS), healthcare settings began experimenting with ways to open lungs. Ventilators did the trick but weren’t equipped to adapt to natural breathing patterns. In the quest to get patients to synchronize with the ventilator – to stop them from taking their own breaths so the ventilator could do the work, and to eradicate related discomfort – medications historically used in the OR (benzodiazepines, opioids, barbiturates, propofol, paralytics) were brought into ICUs. Used for longer periods, these sedatives initially seemed successful and harmless. What we’ve learned in decades since, though, should compel healthcare to reconsider what’s become a cultural norm: the vicious cycle of sedation and immobility.
HARD TRUTHS ABOUT SEDATION
While sedation is certainly necessary for some patients, it’s important to recognize its risks and drawbacks. What we have come to believe is safe, normal, and humane can actually be quite harmful and even lethal.
As touched on above, sedation prevents mobility – grounds for reconsideration in and of itself. Mobility has countless benefits for patients. It encourages physical and cognitive engagement, preserves and restores baseline function, preserves vestibular function, and helps manage anxiety, delirium, and agitation, to name just a few. Failing to mobilize patients in the ICU is an independent risk factor for readmission and death within the first year after discharge.
Beyond its impact on mobility, though, sedation can pave the way for some or all of the following:
- Diaphragm disfunction
- Vestibular dysfunction
- Cardiac deconditioning
- 2% muscle loss per day
- Acute brain failure
- Delirium
- ICU-acquired weakness
- Decreased gut mobility
- Pressure injuries
- Hospital-acquired pneumonia
- Deep vein thrombosis
These conditions can lead to a litany of downstream consequences including prolonged time on a ventilator, falls, tracheostomy or peg tube placements, readmissions, lifelong disability, long-term brain injury, PTSD, constipation or ileus, exercise intolerance, orthostatic hypotension, and mortality.
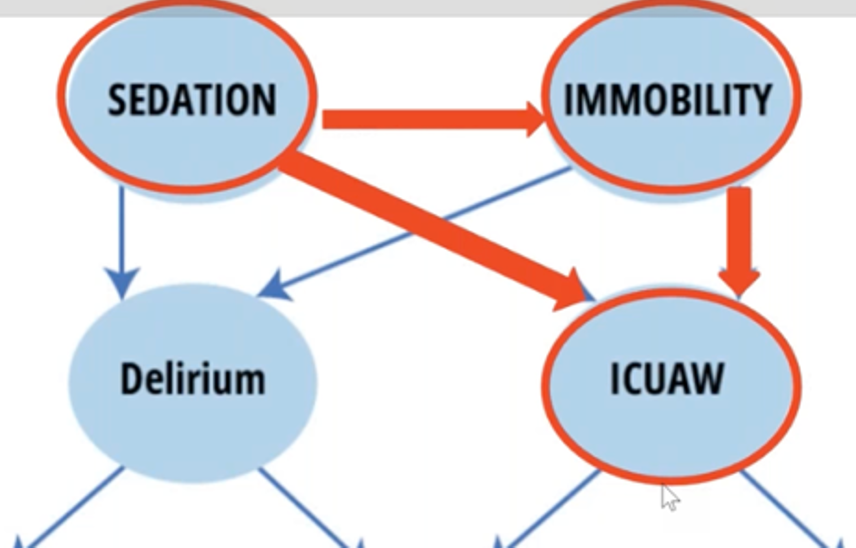
Two of the side effects above are worth unpacking further: Delirium and ICU-acquired weakness, both of which can result from sedation and immobility and both of which put patients at risk for acute or chronic cognitive, psychological, and physical impairments often requiring extensive and even long-term rehabilitation.
DELIRIUM: DANGEROUS AND MISUNDERSTOOD
On average, patients come to the ICU with 11 risk factors for delirium. Add sedation, and these same patients – those on mechanical ventilation especially – see their risk of delirium increase by 126%.

Delirium is widely believed to be transient confusion, likely to disappear once a patient’s health is improved or restored and they’ve returned home and to baseline health.
The reality is far more somber.
Delirium is, in fact, acute brain failure – a neuro-psychotic condition that manifests damage occurring within the brain. Just one day of delirium increases the risk of death by 10%. Just one episode of delirium increases total costs by 40%. It is a life-threatening and life-altering organ dysfunction that:
- Doubles the risk of dying in the hospital
- Triples the risk of death within six months following discharge
- Makes a patient 3.3 times more likely to be discharged to a care facility
- Makes a patient 120 times more likely to experience long-term cognitive impairment that often presents similarly to mild Alzheimer’s Disease and a mild traumatic brain injury
- On average, increases ICU time by 4.47 days and time in the hospital by 6.67 days
- Is a major risk factor for post-ICU post-traumatic stress disorder (PTSD)
Beyond confusion, graphic, vivid, and traumatic alternative realities are common within delirium. When this occurs, the pain a patient would feel in the absence of sedation is twisted into graphic scenarios. One survivor I interviewed spent three weeks under sedation “seeing” babies thrown into a fire and trying to save them – an experience so vivid, real, and prolonged and responsible for such deep psychological trauma that she had documents drafted protecting her from future sedation via DNS (do not sedate) orders.
Other patients have described perceived experiences of torture, organ harvesting, kidnapping, sexual assault, and severe isolation. One survivor spent his time under sedation feeling like his father was cannibalizing him. Years later, he still could not look at photographs of his father.
This all serves to remind us that while we’ve been conditioned to believe that sedation is humane, comfortable, and safe for patients, that is not always the case.
ICU-ACQUIRED WEAKNESS: WORTHY OF AWARENESS
In addition to delirium, sedation and immobility can also lead to ICU-acquired weakness (ICUAW).
ICU-acquired weakness is better described as muscle failure, or dysfunction and atrophy within the muscle and/or related nerves.
At baseline, most ICU patients are already experiencing assault to their muscles upon admission – typically from systemic inflammation, at minimum. Those who are sedated then experience, on average, 30% muscle mass loss within the first 10 days in an ICU, often leading to ICU-acquired weakness. As this occurs, muscles release more inflammatory markers which not only exacerbate muscular atrophy but hit the blood brain barrier, increasing delirium and neurodegeneration. ICU-acquired weakness can be caused and accelerated by additional factors including catabolism and medications like steroids, antibiotics, and sedatives.
Below are some common outcomes stemming from ICU-acquired weakness, all of which are life-threatening or life-altering:
- Tracheostomy resulting from diaphragm and respiratory muscle function weakness
- Long-term acute care hospital or skilled nursing facility placement
- Pressure injuries
- 30% increase in in-patient mortality
- 42% increase in 2-year mortality
- In the first year post-ICU discharge, a 3.6-time greater likelihood of death
- In the first year post-ICU discharge, an average 16.7 unit decrease in physical function domain score. If previously walking independently, a patient may now need to use a walker for prolonged periods. If they used a walker before, they may be in a wheelchair for prolonged periods, if not for the rest of their lives
One recent study of medical ICU survivors found that 66% were unable to stand at discharge. Thirty-six percent still could not stand at three months post-discharge. All in all, these patients experience a 4.2-fold increased risk in mortality.
So what can be done to limit the damage caused by sedation? How can we sedate when medically necessary but implement informed restraint whenever possible?
The ABCDEF bundle is widely regarded as the best means for informed decision-making related to sedation.
ABCDEF BUNDLE
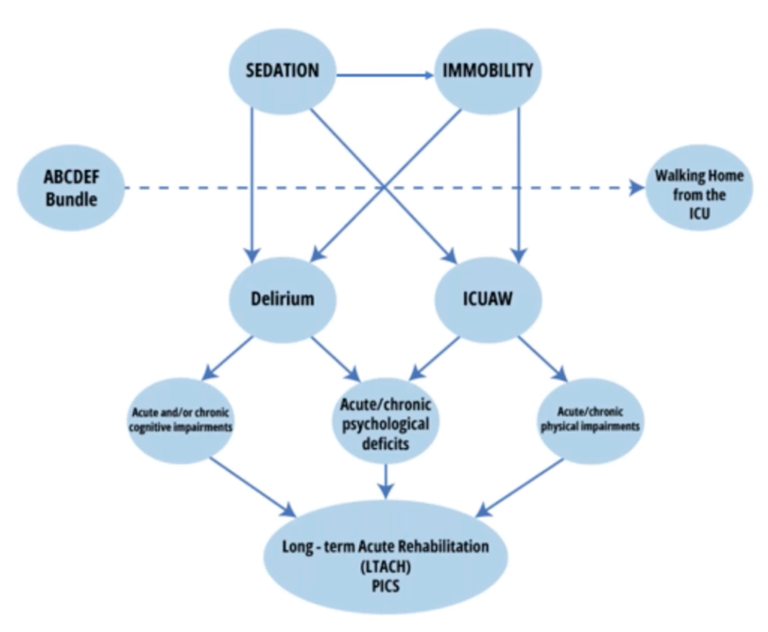
Developed by the Society of Critical Care Medicine in 2014, the Adult ICU Liberation Bundle, also known as the ABCDEF Bundle, is a set of evidence-based guidelines designed to help healthcare settings activate organizational changes that can help facilitate an awake and walking ICU – key to preventing delirium and ICU-acquired weakness, among other sedation-induced complications.
Some of these can appear simple. In the context of ICU, however, and in tandem with the larger bundle, they’re profound. Which is to say: resist the urge to cherry pick. All six interventions in the bundle are interdependent. Only together can they help bring about organizational change.
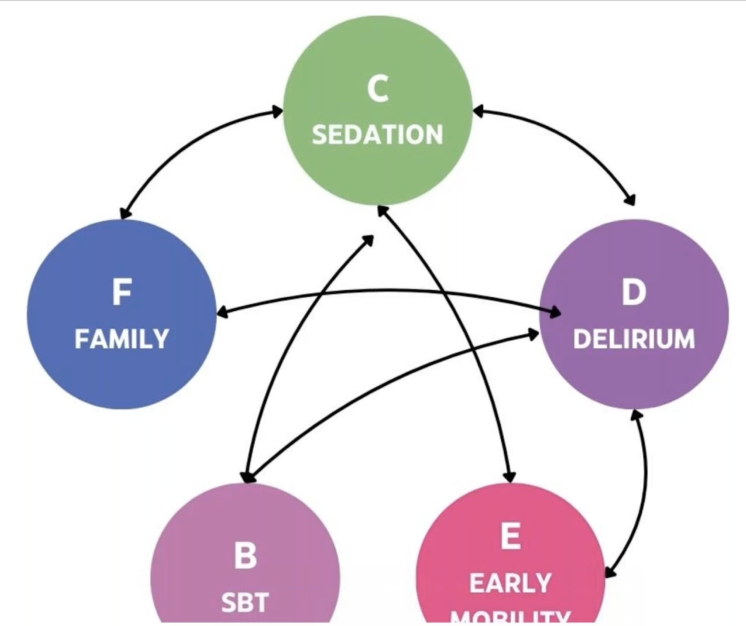
ABCDEF is an acrostic for remembering six key steps:
- Analgesia: Assess, Prevent, and Manage Pain
- Both Spontaneous Awakening Trials (SATs) and Spontaneous Breathing Trials (SBTs)
- Choice of Sedation and Analgesia
- Delirium Identification and Management
- Early Exercise and Mobility
- Family Engagement and Empowerment
(It’s worth noting F – family engagement and empowerment – was added in 2023[1]. Because it came later, it is sometimes missing from the acrostic).
A little more about each of the six:
- Analgesia: Assess, Prevent, and Manage Pain. Historically, any patient on mechanical ventilation was assumed to be experiencing pain and started on fentanyl or another opioid without question. Healthcare standards have begun to evolve to a place of assessing a patient’s patient before prescribing sedatives or painkillers – whenever possible by asking them about their experience. If a patient is coherent and there’s not already an indication for sedation, ask them what they’re feeling and make decisions accordingly.
- Both Spontaneous Awakening Trials (SATs) and Spontaneous BreathingTrials (SBTs). Recognizing that sedation comes with risks, these trials are opportunities to gauge the possibility of removing sedation if not indicated. When and whether this is viable requires separate interventions, or trials, often conducted at separate times. First, a patient is taken off sedation – again, only if not indicated. Remember, mechanical ventilation alone is not an indication for sedation. Separate breathing trials determine whether independent breathing and extubation are feasible. Because these two trials fall under the same letter – B – to fit the ABCDEF acrostic, they’re sometimes misinterpreted as interdependent. Some also assume that an awakening trial needs to happen before the breathing trial because it’s listed first. Neither of these is the case. These trials are independent and can be conducted in any order.
- Choice of Sedation and Analgesia. If there is an indication for sedation, choose the safest sedative at the lowest dose for the shortest duration possible – prosthetics over propofol, for example. Try to keep patients as awake as possible and reevaluate every shift, every day, asking whether the indication for sedation has been resolved and whether something safer could be used. Are awakening and breathing trials viable options?
- Delirium Identification and Management. Prevent, assess, and treat delirium. There are four tactics for accomplishing this: 1. Avidly avoid deliriogenic medications, which cause delirium, 2. Family engagement 3. Get real sleep, and 4. Mobility.
- Early Exercise and Mobility. Beyond its physical and cognitive merits, mobility is key to humanizing patients and their care. Dr. Bill Beninati, LDSH, uses a phrase I love: “Walk when wild, walk with sluggish.” In short, whether an unsedated patient is restless, anxious, and tired or moving and grooving, get them sitting up at minimum and standing and walking if possible.
- Family Engagement. When patients automatically receive deliriogenic medications, they cannot engage meaningfully with loved ones. Family engagement is shown to improve patient health outcomes and satisfaction. Even more, it correlates with better adherence to treatment plans.[2]
This is just the beginning of the conversation. Sedation and related choices by healthcare providers in the quest for an awake and walking ICU is a complex topic worthy of closer examination. Explore it further and earn one free contact hour by listening to the full on-demand webinar.
Kali Dayton, DNP, AGACNP

Kali founded Dayton ICU Consulting, focusing on transforming intensive care units with the “Awake and Walking ICU” model to master the ABCDEF Bundle, evidenced by successful programs across 13 ICUs. She has led over 30 educational programs, empowering staff with the skills to improve ICU experiences for patients and caregivers alike.
Kali also hosts a podcast, “Walking Home From the ICU” which advocates for ICU advancements and patient support through over 170 episodes, further establishing her expertise in the critical care field. This dual engagement in practical application and thought leadership underscores her mission to drive continuous improvement in critical care practices.