Under Pressure: The Physiologic and Bio‑mechanical Value and Realities of Patient Offloading
Offloading – sometimes called mechanical unloading – is the process of reducing force on body tissue by minimizing or reducing pressure or weight. The central tenet of patient positioning, offloading can prevent complications (including pressure injuries) and promote healing in skin and beyond. Below, we’ll unpack the complicated relationship between force and immobility and offer practical suggestions for real-world healthcare settings. Listen to the full on-demand webinar to earn one contact hour.
“Motion is lotion” is a popular phrase among physical and occupational therapists, for good reason: When humans are immobile for prolonged periods, body tissue responds differently to physiological and pathological contacts. Beyond skin-related complications, the absence of standard movement, environmental interaction, and ambulation can lead to dysfunction throughout the body, especially among older patients and those with comorbidities such as peripheral arterial disease:
- Decreased protein synthesis pathways. Downregulation of anabolic pathways such as the mTOR (mammalian Target of Rapamycin) pathway diminishes muscle protein synthesis.
- Mitochondrial dysfunction. Reduced mitochondrial biomass and function in the cell’s powerhouse impairs energy production.
- Altered gene expression. Immobility can lead to changes in the expression of genes related to muscle contraction, metabolism, and growth.
- Muscle atrophy. Also called muscle unloading, muscle atrophy occurs when cells shrink due to decreased protein synthesis and increased protein degradation. Satellite muscle stem cells, crucial for muscle repair and regeneration, may also show impaired activation and differentiation.
In terms of skin specifically: immobility combined with decreased skin tissue tolerance increases the risk of pressure injuries – a critical and costly concern on today’s healthcare landscape. Pressure injuries can be profoundly painful for patients and can introduce a wide range of related negative sequelae, including mortality. An estimated 60,000 deaths are attributed to pressure injuries each year. The incidence rate for pressure injuries in acute care settings (2-%-40%)is the highest of any care environment (e.g. rehabs, nursing homes, and long-term care, by comparison, run closer to 12%).
Pressure injuries are especially common on the sacrum and the heels, with heels accounting for 41% of more progressed deep tissue injuries (DTI). Foot and heel pressure injuries have the highest mortality rates, too, in part because patient ambulation is often restricted – a catch-22 we’ll elaborate on below.
PRESSURE INJURY SUSCEPTIBILITY
As mentioned, a patient’s likelihood of developing a pressure injury depends largely on tissue tolerance, which determines the ability of skin and supporting structures to endure pressure without adverse sequelae (commonly known as complications).
Tissue tolerance is determined in part by skin anatomy, but can also be compromised by immobility, surface pressure, and a wide range of comorbid conditions and circumstances common in acute care (and in the ICU especially). Any of the following can contribute to one’s risk of compromised skin:
- Diabetes
- Vascular disease (such as peripheral arterial disease)
- Nervous system conditions (such as neuropathy)
- Impaired nutrition
- Perfusion issues
- Mechanical ventilation
- Medical devices
- Surgery (especially if >2 hours)
- Moisture (fever, incontinence)
- Low oxygenation
- Length of stay
- Age
- Weight
- Prolonged standing
- High impact activities
- Inappropriate footwear
- Positioning
Below we’ll focus on that last contributor: patient positioning, which is key to offloading & ultimately to pressure injury prevention.
THE POWER AND COMPLEXITY OF PATIENT POSITIONING
Positioning is fundamental to maintaining patient safety and to setting the stage for optimal outcomes. It is defined as the deliberate placement of a patient in a specific posture to aide in one or more of the following:
- Facilitate a procedure
- Promote safety and comfort
- Prevent complications including pressure injuries (pressure ulcers, nerve injury, deep tissue injury, angiosomal occlusion)
- Facilitate recovery, especially after a cardiac event or vagal response
Of note: There’s a slight but important difference between positioning and repositioning. Repositioning is generally understood as the act of adjusting a patient’s initial position every two hours at minimum, or as needed – an industry-wide standard of care integral to preventing skin breakdown. For the purposes of this piece, we’ll use the term positioning to describe both positioning and repositioning except where otherwise indicated.
Whatever the acute goal, positioning should always include efforts to offload – that is, to reduce force on body tissue by minimizing or reducing pressure or weight and/or by varying the number of contact points.This allows tissue reperfusion, reducing the chance of skin injury. However, offloading via patient positioning is more complicated than meets the eye. The most common patient positions in hospital and care environments are supine, semi-Fowler, and Fowler. All three have benefits. In all three, though, a patient’s bony prominences inevitably make contact at various points with the hospital bed or surface. Put another way, patient positioning can be both a strength (prevention agent) and a liability (risk factor, for skin especially), i.e. there is often a bidirectional relationship between positioning and larger health goals. Ambulation is a great example: Ambulation can delay pressure injury healing on the feet and heels in particular; however, a patient who’s not up and moving might be more likely to experience cardiovascular decline.
Provider safety is also a critical part of these conversations. The average patient weight continues to increase. Meanwhile, the medical field continues losing professionals to patient handling-related concerns, stress, and injury. Provider protections need to factor into positioning-related dialogue.
SO WHAT DO WE DO ABOUT IT?
There’s a positioning “Goldilocks” – a point at which both patient and provider experience optimal safety during positioning. Achieving it often involves use of offloading devices that conform intimately to the body’s contours (called enveloping). Envelopment allows for pressure redistribution – that is, it distributes force otherwise incurred by bony prominences onto the musculature and soft tissues and onto a wider area overall, reducing peak pressure.
Offloading devices are not a catch-all, nor are they suitable for every patient at every point. It’s important to consider:
- Patient preference. If a patient is awake, alert, able, and willing to participate in discussions, work to find a balance between what they want and their risk.
- Anatomical differences. Many individuals with sharp co-foot or contractures have altered bony prominences which need to be accounted for in device use and positioning.
- Braden subscores. The Braden Scale assesses a patient’s pressure injury risk factor; a patient’s Braden score should be central to related decision-making.
- Patient activity and mobility level. Will devices allow the advisable amount of movement and ambulation?
- Clinical condition and tolerance (agitation, muscle spasms, kicking, scooting). Is a device likely to stay in place? Will the patient physically co-exist with it?
- Device availability. Is an item likely to be stocked, ready, and reliably available when you need it?
BEST PRACTICES FOR A COMMON OFFLOADING DEVICE: SUPPORT WEDGES
A wide variety of options can assist with patient positioning and therefore offloading:
- Prophylactic and other preventative dressings
- Offloading boots
- Support wedges
- Pillows
Of the items above, support wedges are one of the most common. Typically triangular-shaped and made from high-density foam, inflatable material, or other flexible materials, support wedges go a long way toward helping healthcare providers optimize patient positions most likely to advance positive health outcomes. They’re designed to provide firm, stable support for the body and allow for a wider range of positions than what could not be achieved otherwise.
Support wedges are uniquely helpful in achieving and maintaining the 30-degree lateral tilt – a position that offloads the sacrum and coccyx by shifting patient weight onto the larger muscle group of the buttocks. This position is widely recommended across international guidelines.
A few suggestions for use of support wedges:
- Position wedges above and below bony prominences. While softer than support surfaces, support wedges should nonetheless remain out of contact with high-risk bony areas.
- If able, assess patient skin every time you reposition devices. Be sure to document findings, key to protecting yourself in the event of legal action.
- Consider the angle of the head of the bed. When a patient is in it, the head of a bed should be raised no more than 30 degrees. A higher angle can increase pressure on the sacrum, causing the patient to slide down, increasing shear risk. If a patient needs the head of the bed elevated for respiratory issues, dysphagia, or other competing medical priorities, note that reasoning in your charting.
- Use proper lifting techniques. Always use proper moving and handling aids (such as slide sheets, lifts, and air-assisted devices) when positioning patients. Avoid dragging or sliding, which creates friction and shear forces. Teach patients to protect themselves, too. If a patient is dragging themselves across a bed, for example, it might be an opportunity to demonstrate and explain the value of lifting. This can be especially valuable for patients approaching discharge, who will soon be creating habits at home.
OFFLOADING DEVICE PERFORMANCE, ASSESSMENT, & MAINTENANCE
When offloading devices lose their integrity and therefore their effectiveness, it directly undermines the entire proactive prevention strategy. Patient safety is compromised. Clinicians are forced into reactive mode as they address conditions that could have been prevented.
This is not a hypothetical concern. One rigorous bio-mechanical study of wedges’ clinical durability was designed to simulate intense demands of the hospital environment: real-world exposures, 72-hour q2h turning protocol, and body mass simulated by a 350-pound bariatric mannequin.
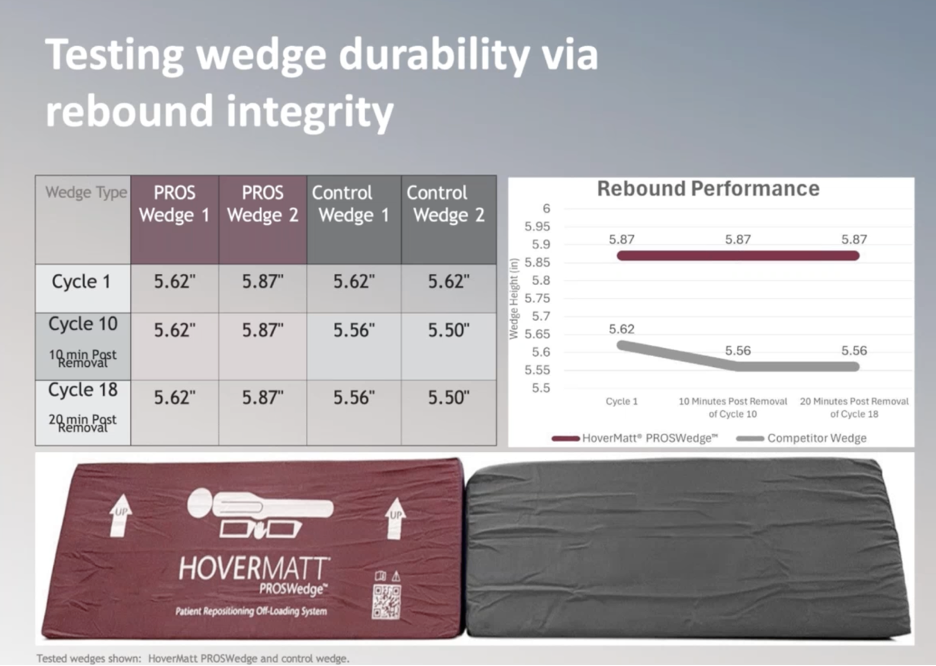
After the first repositioning cycle, all wedges returned to their original shapes. After 10, then 18, cycles, wedges began diverging in their ability to hold up to pressure. A decrease in performance is known as material fatigue – the phenomenon wherein material loses its structural integrity, original shape (sometimes referred to as memory), and functionality after some period of repeated loading and unloading.
The loss in integrity observed in this study, it turned out, directly correlated to foam quality. Higher quality foam lasted longer and performed better over its lifetime.
In light of findings, material fatigue prevention is understood to be two-fold:
Clinicians and healthcare systems must continuously assess offloading devices already in-house. This can be challenging for several reasons including the fact that breakdown is often incremental and subtle. Clinical staff must therefore be educated and on the lookout for indicators of material fatigue, which allows for timely device replacement. Attention should extend beyond visual wear to systemized testing for performance-related indicators: How do devices hold up over their clinical lifespan, and how long is that lifespan? How do they hold up when exposed to moisture, like when patients become diaphoretic or incontinent? For how long are they effective? With wedges, can they sustain the optimal 30-degree tilt that keeps patients from rolling down in bed?
Secondly, healthcare systems should consider foam quality, and therefore performance, when making purchasing decisions. Providers need to proactively advocate for procurement policies that prioritize products’ evidence-based durability and long-term performance over initial acquisition costs. If something is shown to be safe, effective, and more durable than other alternatives, it’s essential to prioritize it over products with lower price tags.It’s worth repeating: Offloading via patient positioning and repositioning can reduce pressure injury occurrence and severity and lead to stronger patient outcomes. Right-fit devices play a huge role.
Eager to learn more about improving offloading practices in your acute care setting? Earn one free contact hour by listening to the full on-demand webinar.
Dr. Laura Swoboda, DNP, APNP, FNP-C, FNP-BC, CWOCN-AP, WOCNF

Dr. Laura Swoboda is a translational scientist, family nurse practitioner, and wound specialist in Milwaukee, Wisconsin. They represent the US as a diplomat on the International Skin Tear Advisory Panel, serve as treasurer for the AAWC, are on the board of directors of the Save a Leg, Save a Life Foundation, and are active on various committees for the NPIAP, Wound Healing Society, WCCC, Alliance of Wound Care Stakeholders, and the American Heart Association’s Peripheral Arterial Disease Collaborative. They remain committed to health equity and volunteer at the local, regional, national, and international levels to increase access to quality healthcare.