Caring for Patients with Bariatric Disease in the Perioperative Setting

Rates of Class 3 obesity are on the rise, necessitating efforts to improve bariatric care, including bariatric perioperative care. The recommendations below help ensure dignity, safety, and optimal health outcomes for patients with high BMI as well as the safety of perioperative clinicians. Listen to the full on-demand webinar to earn one contact hour.
Bariatric nursing is the practice of providing holistic care to patients with Class 3 obesity, a complex chronic disease in which an individual has a body mass index (BMI) of 40 or higher. According to the Centers for Disease Control, nearly 10 percent of American adults have Class 3 obesity.
Patient handling and mobility – that is, safely lifting, transferring, positioning, and otherwise moving patients – is a pervasive challenge when caring for bariatric patients. Additionally, patients with Class 3 obesity are at heightened risk of health conditions including diabetes, heart disease, various cancers, and osteoarthritis. These factors complicate care in any healthcare setting and particularly in surgical settings, where space and time are often limited and where stakes are uniquely high.
Below, we’ll identify areas of perioperative risk for patients with high BMI. From there, we’ll review equipment considerations, safe positioning techniques, and patients’ physiologic needs in all three parts of the perioperative setting: pre-operative, intra-operative, and post-operative.
But first, a general note on caring for patients with high BMI:
The World Health Organization and other national, international, medical, and scientific societies recognizeClass 3 obesity as a multi-causal condition, more complex than historically recognized.Still, weight bias continues to pervade healthcare settings, with dire results. Negative attitudes by healthcare providers have been cited by bariatric patients as a reason they avoid medical treatment and preventative screenings, potentially contributing to adverse health outcomes. The onus is on healthcare providers to help offset these troublesome trends by providing better support for the Class 3 obesity population. As such, the suggestions below are both practical and holistic in nature, designed to optimize perioperative settings and contribute to whole-person care for patients with high BMI.
DEVELOPING AN INDIVIDUALIZED PLAN OF CARE
A collaborative culture of safety is the pursuit of sFor all surgical patients, perioperative team members must identify specific patient liabilities, including propensity for positioning injury, prior to surgery. This information informs an individualized plan of care – a custom plan addressing the patient’s exact needs, procedural specifics, medical history, risks, and preferences across the surgical journey.[1] An individualized plan of care is acutely essential for patients with high BMI, for whom there is an increased risk of premature mortality in addition to practical challenges. Patient assessment should include a clear understanding of and resource allocation (including equipment decisions) related to:
- Patient weight
- BMI
- Body habitus
- Current skin conditions and skin integrity
- Current musculoskeletal nerve function
- Chronic medical conditions
- Ability to tolerate the procedure positioning
- Procedure access site and IV sites
- Procedure length
- Circulatory respiratory system function
- Protection of the neuromuscular and skin integrity
- Environmental conditions including temperature and humidity
A careful review of these variables won’t just elevate patient care and outcomes – it also sets the stage for safer, more seamless experiences for perioperative staff.
PRE-OPERATIVE SETTINGS
For many patients, check-in areas, waiting rooms, and assessment spaces are their first impression of the perioperative setting. These pre-operative spaces should be inclusive, welcoming to the full range of body types, ranges, and sizes – yet, too often, fail on some or all fronts.
Healthcare professionals need to look at pre-operative spaces and ask themselves the following questions:
- Can existing seating accommodate patients of varying weights and abilities? Consider the patients (and their family members and care teams) who come through the doors daily. Orthopedic patients often need elevated chairs due to musculoskeletal limitations. Wider chairs provide comfort and dignity to patients with obesity who might not be able to use standard-sized seating.
- Can pre-operative assessment spaces accommodate patients with obesity? Beyond suitable access and seating, does a patient with high BMI have ample space to comfortably change into a gown?
- Are patient gowns available in a wide range of sizes?
- Are scales located in an area that offers privacy? Are scales’ weight capacities sufficient for all patients?
Patients are typically transferred from pre-operative areas to the operating room (OR) by a stretcher or wheelchair. On occasions when a patient is ambulatory, and when it’s deemed safe to do so, they might walk. All these transport options require certain considerations for patients with high BMI:
Stretchers:
- Stretchers are ideally motorized to reduce exertion required by staff.
- Stretchers must be set to the correct height for transporters. Ideally bed height reaches the middle of the transporter’s core. In the event of multiple transporters, defer to the height of the person driving the stretcher.
- Stretchers (including motorized stretchers) should be accompanied by at least two transporters whenever possible. This not only reduces necessary exertion; it allows one team member to swipe badges for access to restricted areas and/or hit buttons to open doors, reducing stop-and-go that can cause patient discomfort and even injury. Add more transporters as needed based on a patient’s weight and body habitus, or as dictated by a healthcare setting’s specific transportation hurdles (long and irregular corridors, for example).
- Ensure that all transporters know how to adjust stretcher settings and how to properly adjust, move, and use the stretcher overall.
- Avoid stretcher-related shortcuts, like using the CPR quick release or head-up CPR (HU-CPR) function in specialized stretchers for reasons other than its intended use. Using HU-CPR to raise a bed puts the head of the bed at risk of falling back if it does not properly lock.
Wheelchair
- Ensure that bariatric wheelchairs are available and utilized.
- Ensure that patients wear slip-free footwear – vital if they need to stand and/or walk during transfer to the operating table but advisable regardless.
- Have stairs available to assist the patient onto the operating table if needed.
Walking
- Again, ambulatory patients must wear slip-free footwear.
- Confirm that the pathway to the surgical area is clear of tripping hazards.
- Have a staff member escort the patient. Confirm that this clinician is prepared and equipped to provide support in the event of instability or a fall.
- Have stairs available to assist the patient onto the operating table if needed.
Once a patient reaches the operating room, they’ll need to be transferred to the surgical operating room table (sometimes called an operating room bed). For patients transported to the OR via stretcher, this will require a lateral transfer.
Lateral transfers, like all transitions from one horizontal surface to another, are complex with any patient. They are especially complex with patients with high BMI, for several reasons: High patient weight increases the likelihood of accidents and patient injury including skin shearing. Gels, strips, and other anti-slip adhesives applied to the OR table to decrease patient sliding and movement during the procedure can become barriers to transfers onto the table. Breathing challenges common among the bariatric population must be considered and accommodated. Furthermore, many patients with high BMI have limited mobility, reducing or even eliminating their ability to participate in the transfer.
The factors above also introduce risk (notably, musculoskeletal injury risk) for clinicians. These risks are amplified when clinicians invite patients to lean on them for support, or when they use draw sheets to ostensibly help movement along – a choice that is never advisable. Remember, draw sheets are not your friend and should never be used for patient movement, handling, or positioning.
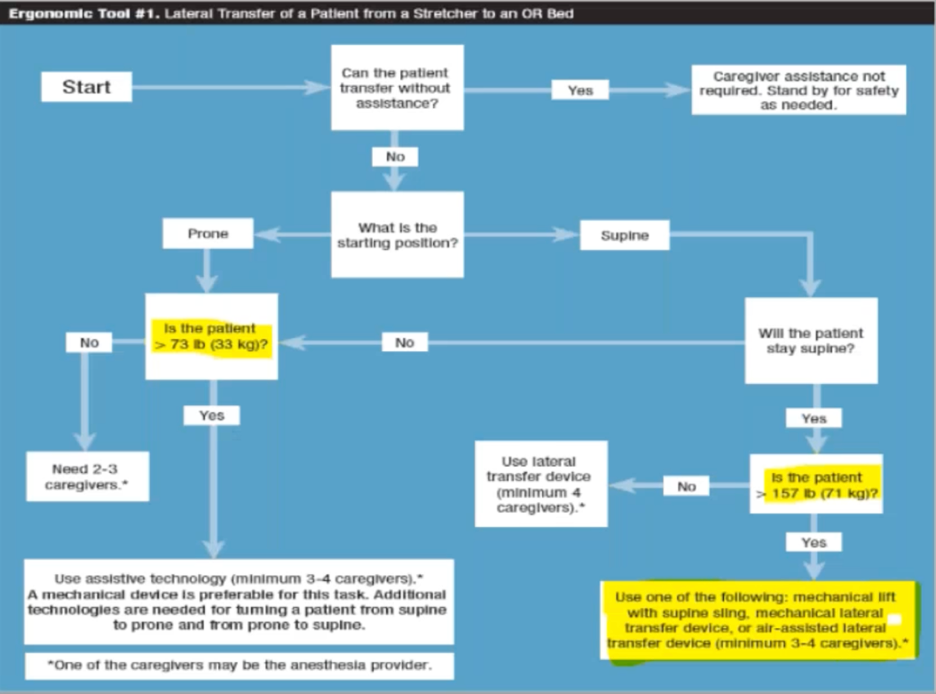
A far safer tool for patient movement is a weight assistive device, such as a lateral transfer device. Weight assistive devices are recommended by the Association of Perioperative Registered Nurses (AORN) in any scenario in which a caregiver is required to lift more than 35 pounds. It’s worth noting that weight assistive devices are superior to simply enlisting more team members to help with a transfer. No matter how much care and attention clinicians offer, risk of injury for all parties increases as patient handling teams expand. Inflatable air-assisted lateral transfer devices are increasingly favored over mechanical lifts, sliding boards, and slings (which are rare in ORs) not only for their ease of use but the fact that they are much more comfortable for patients and can remain beneath a patient for the duration of a procedure. AORN resources, like the flowchart below, offer guidelines for safe patient handling and mobility across a wide range of OR scenarios and variables. This flowchart leads to scenario-specific recommendations for lateral transfer of a patient from a stretcher to a surgical table:
If transfer technology is not available in your facility or perioperative setting, it’s something to push for and consider, especially if working with a high rate of patients with Class 3 obesity.
INTRA-OPERATIVE SETTINGS
A key difference between pre-operative and intra-operative settings is that, in intra-operative settings, patients are no longer awake. Anesthesia administered on the OR table renders them unable to assist with positioning. This elevates the importance of choosing compatible operating room equipment.
When choosing and preparing OR equipment for patients with high BMI, remember: All medical equipment includes manufacturer’s instructions for use (IFU). Be sure to check these IFU guidelines for limits related to patient weight as well as height and other considerations. The need for IFU verification is highlighted in a few scenarios outlined below; however, IFUs should be consulted in all equipment-related decisions.
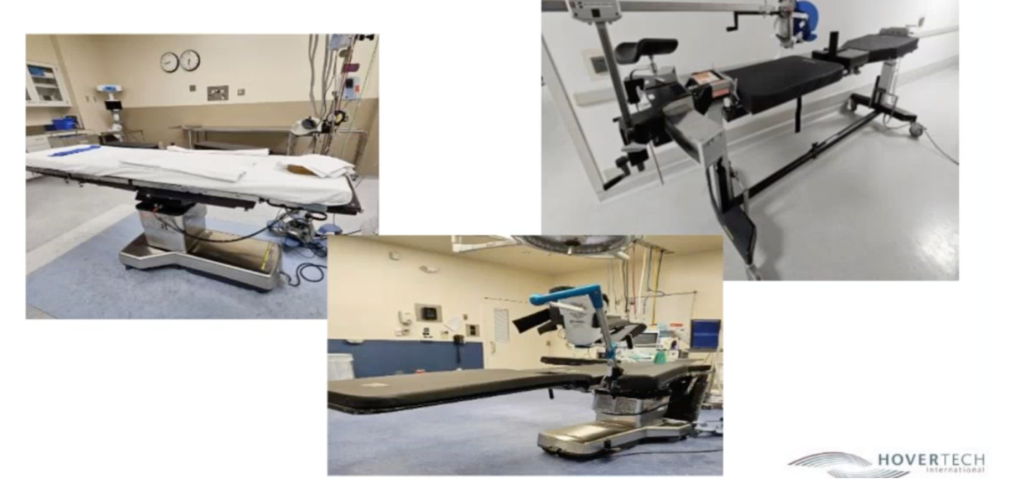
There are three major categories of surgical operating room surgical tables, each with unique functionalities:
- General surgical table (left photo)
- Radiolucent imaging table (center bottom photo)
- Orthopedic table (right photo)
When choosing between OR tables for patients with high BMI, consider the information gathered during the patient assessment relative to not only the table’s weight capacity but the following:
- How will the patient be positioned on the bed, and is this position compatible with the chosen table? On general surgical tables, for example, most of the patient weight should be situated atop the support column/base.
- Some OR tables have sliding elements or other moving parts and attachments that need to be manipulated. Is this manual manipulation feasible considering the patient’s specific profile and needs?
- What is the weight of the table itself? Some specialty tables weigh close to 1000 pounds. The combined weight of the patient and table must be within reach of a team’s exertion capability, as beds may need to be moved, unlocked, and rotated (in arteriovenous fistula procedures, for example).
- Will the bed mattress provide sufficient support and padding? Is there risk that the mattress will bottom out, increasing the likelihood of pressure injury development? For patients with Class 3 obesity, high specification or reactive foam is ideal.
- Is the table wide enough to keep the entirety of the patient’s body on the bed? Most operating room tables are 20 inches wide, which can prove insufficient in supporting the full width of some patients. If a wider bed is necessary but unavailable, are bariatric extenders compatible and available? Keep in mind: Bariatric extenders add distance between the surgical team and procedural site, sometimes reducing surgical exposure. Will this prove detrimental?
In many cases, stirrups (also known as leg supports) are also needed. After a patient is sedated, clinicians are typically responsible for positioning a patient’s legs into the stirrups. Per AORN guidelines, patient legs should be placed into stirrups simultaneously to reduce risk of patient injury such as thermal nerve damage, hip dislocation, low back strain (including torsion of the lower lumbar spine), and sciatic nerve injury. For patients with high BMI, two or more clinicians per leg might be required.
In choosing which stirrup to use for patients with high BMI, ask yourself:
- Are the stirrups pneumatic? Pneumatic stirrups use gas-spring technology to assist with lifting, positioning, and reducing nerve pressure.
- What is the weight capacity of the stirrup? Many cap out at 350 pounds. Note that stirrup weight capacity refers to total patient weight, not per-leg weight. Bariatric stirrups are available.
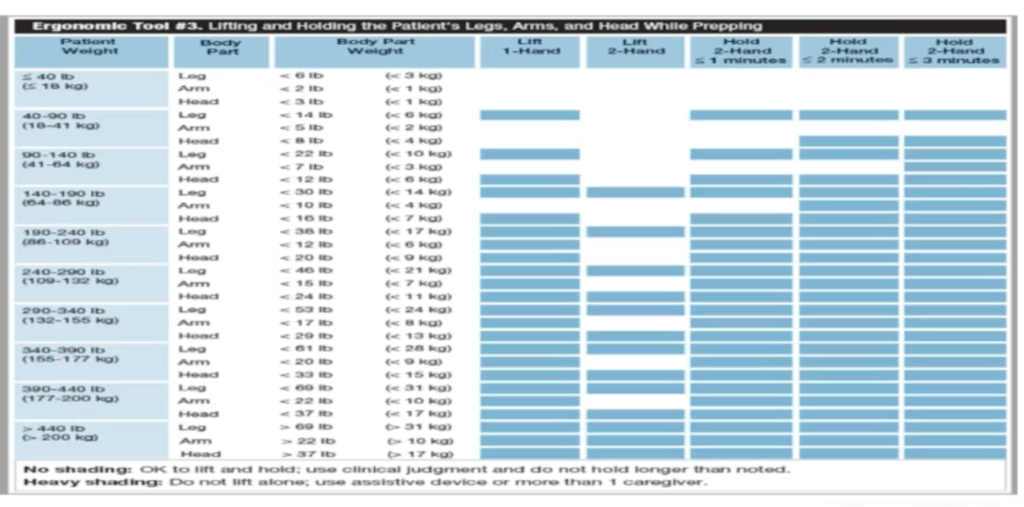
Limb preppers are also common in operative settings. Designed to hold patient arms, legs, and extremities so staff can clean the surgical site and give surgical access, these also have weight limitations that need to be checked. Note that AORN provides guidelines for lifting and holding a patient’s legs, arms, and head while prepping:
Moving beyond equipment to bariatric patient positioning: Considerations also exist for specific medical/surgical patient positions. The specificity and risks of each underscore the importance of attention, control, and (whenever possible) minimized patient movement with all patient populations, but especially when positioning patients with high BMI:
Supine. Because arms are positioned on arm boards extended more than ninety degrees, there is risk in supine position of damage to the brachial plexus nerves.
Trendelenburg. Extreme caution is needed when placing a patient with high BMI in the tilted, head-down Trendelenburg position, a variation of supine used to move abdominal organs upward to improve access to the pelvic and lower abdominal region.[1]Patients with Class 3 obesity and heart, lung, liver, kidney disease are at increased risk for ineffective oxygenation in Trendelenburg. In terms of cardiovascular considerations, Trendelenburg increases central venous, intracranial, and intraocular pressure. The prolonged head down position inherent to Trendelenburg also causes swelling to the face, larynx, and postoperative upper airway, increasing risk of obstruction. Like all positions in which the head is at a different level than the heart, the effect of the hydrostatic gradient on cerebral artery and venous pressure should also be carefully considered and monitored. Steep Trendelenburg – defined as a patient head-down angle exceeding 35 degrees – is particularly risk-laden, resulting in greater arterial blood CO2.
Lithotomy. Another supine position, in lithotomy a patient is on their back with legs raised and situated in stirrups. Hips and knees are flexed between 90 and 120 degrees and thighs rotated externally. When legs are elevated in lithotomy, preload increases, causing transient increase in cardiac output, and, to a lesser extent, cerebral venous intracranial pressure. The abdominal viscera displace the diaphragm, reducing lung compliance and potentially decreasing tidal volume. There are concerns about the saphenous nerves, coronial nerve, femoral nerve, and obturator nerve because of how the legs are positioned. Used commonly in urology and OBGYN, lithotomy necessitates a particularly high number of patient movements, due in large part to the need to slide the patient down and up the bed to get them into and out of the position and to align stirrups accordingly.
Fowler’s Position. Also known as shoulder procedure or beach chair, in Fowler’s Position the head is elevated between 45 and 60 degrees[2] with knees straight or slightly bent – a position that improves oxygenation and alleviates breathing efforts because head, neck, and shoulder elevation allow for optimal airway alignment (Fowler’s is sometimes utilized when a patient is unable to tolerate a supine position for anesthesia). While seemingly more straightforward than the positions above, Fowler’s Position introduces increased risk of skin injury from shearing and sliding and ushers in an increased risk of deep vein thrombosis (DVT) formation on lower extremities. Like lithotomy, Fowler’s Position requires a high degree of repositioning to bring a patient safely into the desired position and back again once a procedure is complete. It also requires raising and lowering the bed, which typically occurs manually – another instance in which total equipment and patient weight, and the capacity of the caregivers, needs to be carefully calculated.
Prone. Many surgical procedures (including spinal, rectal, and gastroenterology procedures) require prone position, a face-down position in which a patient lies on their abdomen.[3] In prone, pressure is exerted onto the abdomen, reducing blood flow to the inferior vena cava, corneal abrasions, edema to the face, nerves, injuries, pressure on chest, knees, toes, etc. Prone also requires many movements and steps. The stretcher needs to be raised up to the bed. Then the patient needs to be turned onto the positioning OR table and repositioned as needed. This high degree of necessary motion and risk command the utmost in attention and right-fit devices.
Lateral. Lateral position, in which a patient is situated on their left or right side with the operative site facing up, is used in a wide variety of surgical procedures. Although this position improves breathing and drainage and can prevent aspiration, it requires use of padding on bony prominences to prevent development of pressure injury. Beanbag or backpack devices are sometimes used to position a patient in lateral.
Another factor across all patient positioning is anesthesia risk mitigation. Patients should be positioned for induction of anesthesia per the anesthesia provider’s instructions. If unable to tolerate supine position, a head-elevated position is likely, as these positions can facilitate optimal airway alignment. Wedge-shaped positioning devices that support the head and shoulders are often essential to achieving these positions. Keep in mind: these positioning devices need to be removed before the procedure can begin and, in many cases, need reinserted beneath the patient at the end of the procedure for safe extubation.
POST-OPERATIVE SETTINGS
Patients discharged following a procedure nonetheless need to be transported by wheelchair to a vehicle, which brings up some of the same considerations that were addressed pre-operatively: Are bariatric wheelchairs available to offer suitable weight capacities and comfort for patients with higher weights?
Patients who are not discharged to home the same day of their procedure are often transported to a post-anesthesia care unit (PACU), then to a patient room where they’ll need to be transported from a stretcher to the hospital bed (if unable to help themselves). Lateral transfer devices including air-assisted devices can again help in these scenarios, in which there are often fewer clinicians available to help than in the OR.
Maintaining the dignity and safety of a patient with high BMI must remain a high priority throughout the perioperative setting. Eager to learn more about ways to improve bariatric perioperative care? Earn one free contact hour by listening to the full on-demand webinar.
Shosha M. Beal MSN, RN, CNOR, CSPHA

Shosha is a Perioperative Nurse Educator based in Lewiston, Maine, currently serving at Central Maine Medical Center. She earned her Bachelor of Science in Nursing from Western Governors University and brings diverse clinical experience. Throughout her career, Shosha has served as a Registered Nurse and Clinical Safety Specialist, with a strong focus on perioperative education and patient safety initiatives.