Cath Lab Safety Essentials: Protecting Patients and Ourselves

Cardiac catheterization laboratories (often called Cath Labs or CCLs) are high-stakes environments for both patients and medical teams. Catheterization lab professionals are advised to pursue a collaborative culture of safety – a proactive and ongoing approach that plans for risk in accordance with evidence-based practice. Learn more below about how to achieve a collaborative culture of safety. Listen to the full on-demand webinar to earn one contact hour.
Designed to diagnose and treat cardiac and vascular conditions, cardiac catheterization laboratories are prepared with advanced medical equipment and a team of medical staff. Interventional cardiologists, as well as nurses and technologists (often serving multiple roles – circulator, scrub, monitor, etc.), are invariably present during procedures. Medical fellows, cardiothoracic surgeons, anesthesia teams, and other ancillary individuals (medical device company representatives, for example) also are often in the mix. The high number of players and moving parts underscores an important point: While catheterization lab procedures are minimally invasive, they’re nonetheless advanced and high-risk for several contributing reasons.
For one, cardiac catheterization lab procedures require vascular access, either venous or arterial (sometimes both).
Fluoroscopy and radiation are key components, necessary for angiography. Once contrast is injected, radiation is used to achieve real-time imaging.
Furthermore, catheterization lab patients typically receive sedation (most often moderate sedation).
Consider the added fact that many Cath Lab patients present with comorbidities and unique medical histories, and it’s easy to understand why a collaborative culture of safety is critical.
DEFINING AND ACHIEVING A COLLABORATIVE CULTURE OF SAFETY
A collaborative culture of safety is the pursuit of safer environments through shared information and responsibility[1] in accordance with best standards and evidence-based practice. Boiled down and stated plainly, it is the philosophy that safety is everyone’s responsibility. Emphasis on everyone. Regardless of experience, education, or title/role, every medical professional is called to proactively uphold safety, not only for the wellbeing of patients, but for their own protection and that of the entire medical team.
At a high level, a collaborative culture of safety involves the following:
- Communication. Essential to any good team, communication is especially critical in CCLs and surrounding areas due to their unique spatial and logistical realities. In CCL suites, control rooms (sometimes called monitoring rooms) are outside of the procedural area. Team members must therefore communicate not only with fellow professionals inside their respective rooms, but also with those on the other side of the leaded glass window. Closed-loop, concise, and clear communication across and within each of these settings is vital.
- Situational awareness and monitoring. Team members must actively and continually scan and assess a situation to gain and maintain an understanding of what’s happening – with oneself, fellow team members, the patient, and the progress towards the procedural goal. This leads to the third, and arguably most challenging, tenet:
- Cross-monitoring. A harm reduction strategy, cross-monitoring is the act of scanning the situation and intervening as needed. Say, for example, a team member preparing to enter the procedural room isn’t wearing a shielding apron, or a tool isn’t sterilized. Anyone who notices must speak up – again, regardless of rank or other factors that might theoretically deter such assertion.
Drilling down further, mitigating and preventing risks specific to the cardiac catheterization lab also involves the following precautions:
PRE-PROCEDURAL CHECKLIST AND TIME-OUT
The pre-procedural verification safety checklist set forth by the Joint Commission must be reviewed and agreed upon in advance of all surgical procedures. This checklist aims to protect against never events (wrong access site, wrong procedure, wrong patient) and a wide variety of other procedural missteps and pitfalls.
In catheterization lab procedures specifically, the pre-procedural checklist put forth by the Society of Cardiovascular Angiography and Interventions must additionally be reviewed and agreed upon by all involved professionals. Among its major components:
- Right patient, procedure, site considerations. Some of these checklist items are familiar: Do we have the correct patient? Are we performing the correct procedure? From here, the Society of Cardiovascular Angiography checklist becomes specific to the task at hand, focusing on safety components, contingency plans should complications arise, and whether contraindications or special considerations exist in relation to access site selection.
- H&P, History (HX) of PCI/CABG, allergies. Ensure access to patient history and physical that is both updated and comprehensive – standard protocol, but particularly vital in catheterization lab procedures where history of Percutaneous Coronary Intervention (PCI) and/or Coronary Artery Bypass Grafting (CABG) is essential knowledge. Patient allergies should also be indicated – most critically, allergies related to contrast, as these require pre-medication and other considerations.
- Recent medications (heparin, acetylsalicylic acid, other anticoagulants). Like allergies, all medications are ideally noted, especially those affecting bleeding times or hemostasis. Vascular access, after all, introduces the risk of bleeding.
- Informed consent, advanced directives, code status, sedation considerations. Ensure receipt of directives including Do Not Resuscitate (DNR) or Do Not Intubate (DNI), and clarity on whether these code statuses are revoked or sustained in the catheterization lab.
- Bleeding risks, laboratory values, baseline ECG. Confirm receipt of all other information, and especially anything that would contribute to additional bleeding risk. In terms of lab values, the catheterization lab team is specifically interested in PT/INR (Prothrombin Time/International Normalized Ratio), H&H (Hemoglobin and Hematocrit), and baseline renal function which could be impacted by contrast.
The pre-procedural safety checklist goes hand in hand with the time-out, but it’s important to note that the two are independent and different undertakings. Whereas the checklist is reviewed outside the catheterization lab, time-out occurs inside the lab, just before sedation is administered and before vascular access is obtained. Time-out helps a team communicate and identify patient risk by reviewing three major areas:
- Right patient, procedure, access site?
- Equipment needed, allergies, pre-medications? Do we have the proper equipment for the procedure at hand? This includes emergency equipment and medication and equipment specific to verified or suspected allergies. Has a patient been pre-medicated (if necessary)?
- Any special considerations?
Like checklists, time-outs end and the procedure proceeds only after all parties verbally agree.
RADIATION SAFETY
The increase in minimally invasive catheterization lab procedures in recent years offers many net benefits. However, this rise in fluoroscopy use brings an increased risk of radiation exposure – not only for patients, but for anyone in the procedure room.
Whereas patients are more likely to suffer direct exposure, radiation exposure risk among catheterization lab medical professionals is more likely occur via scatter, which is secondary radiation exposure that occurs when a beam is deflected. Risk of radiation exposure of any type and by all parties is highest during valve and peripheral vascular procedures, which require more time and therefore more radiation.
To offset these risks, catheterization labs should employ both passive and active radiation prevention and safety measures. Passive protection includes shielding, drapes, and protective equipment. Active protection in this context refers to action taken to increase awareness and quantifiably reduce radiation used: Education and radiation dose monitoring, for example, and steps taken to ensure dose accuracy. A guiding philosophy in radiation exposure prevention is the ALARA principle. ALARA stands for As Low As Reasonably Achievable – that is, the commitment to keeping ionizing radiation doses to the minimum levels possible without jeopardizing the intended imaging goal. This is a regulatory requirement in many fields that mandates actionable measures around time, distance, and shielding:
- Time. In the context of ALARA, time refers to the goal of using fluoroscopy for the least possible amount of time needed.
- Distance. The further an individual is from a radiation source (x-ray tube, for example), the lower the risk of radiation exposure, including risk of scatter. Keep operating tables high and image intensifiers low to reduce risk. Robotic-assisted PCI is an emerging technology that allows medical teams toworkfarther away from patients, and therefore farther from radiation, with the added benefit of letting them sit while working. Robotic-assisted PCI has been shown to offer a mean exposure reduction of 95.2 percent.
- Shielding. Shielding refers to vital protective equipment: lead skirts, vests, radiation goggles with side panels, radiation safety caps, RADPAD® and related products,[2] and thyroid collars. Emerging lead-free options include the Rampart M11128, a shielding device with multiple access points that creates a protective wall between the patient and their interventionalist, theoretically reducing or even eliminating the need to wear lead. Eggnest™ XR is another rising option. A modular lead-free shielding system fully integrated into the procedural space and workflow,[3] Eggnest™ XR reduces the scatter exposure risk without interrupting workflow.
Other radiation exposure prevention practices include varying beam angles, positioning patients in a manner that keeps extremities out of direct reach of the beam, and use of dosimeters. Real-time dosimeters are especially valuable, letting individuals know in the moment whether exposure is high and action needs to be taken. Fetal dosimeters are available for those who are pregnant or might be pregnant.
ERGONOMICS AND PATIENT POSITIONING
Lead-free radiation protection and robotic-assisted systems have an added benefit beyond radiation exposure prevention: they can help offset orthopedic risk.
Orthopedic complications, including musculoskeletal injury and ergonomic issues, are common occupational hazards among cardiac catheterization lab staff. The weight of lead-based personal equipmentis the leading contributing factor, but not the only one. Cath Lab professionals are known to stand in one place and position for extended periods engaging in repetitive movements and heavy lifting, often in relation to handling and moving patients. The low temperatures maintained in catheterization labs can exacerbate these risks. Because team members’ muscles are not warm, musculoskeletal health is compromised. However, opportunities do exist to offset ergonomic risks to catheterization lab medical providers:
- Use low weight aprons. Lead-free aprons are significantly lighter than lead options.
- Optimize posture. Bending, slouching, and straining eyes to look at a procedural site or screen are common in catheterization labs and contribute to posture issues that can lead to orthopedic problems.
- Exercise regularly. Cardiovascular and strengthening exercise can go a long way toward preventing workplace injuries.
- Slide sheets and air mattress transfers devices. By decreasing the exertion necessary to move and reposition patients, slide sheets or air mattresses can significantly offset related musculoskeletal risks. Air mattresses have been shown to reduce the force needed to handle, transfer, and reposition patients by up to 90 percent. They also make the process safer and more comfortable for the patient. Another benefit of slide sheets and air mattress transfer devices: they can remain under a patient for extended periods, easing and helping mobilization and repositioning until the patient reaches their final destination.
CONTRAST-INDUCED ACUTE KIDNEY INJURY (CI-AKI)
Contrast-induced acute kidney injury (CI-AKI) is the third most common cause of hospital-acquired acute renal failure. CI-AKI can be caused by contrast, with risk of CI-AKI occurrence increasing by 12 percent for every 100 milliliters (mL) of contrast administered. In longer cardiac catheterization procedures, several dosages of 100 mLs are not uncommon. The Kidney Disease Improving Global Outcome (KDIGO) states that if a patient has an increase in creatinine (Cr) by 0.3 mg per deciliter (dl) or an increase by 50 percent from baseline, they meet the criteria for contrast-induced acute kidney injury. Ongoing monitoring and attention are therefore key. Abide by the following measures:
- Know the CI-AKI risk factors. These include modifiable risk factors such as hypotension, hypovolemia, anemia, and pre-procedural hyperglycemia, among a host of other signs found here.
- Pre-, intra-, and post-procedure hydration. Hydration is essential to decreasing CI-AKI risk, in large part because it flushes out contrast. Hydration should occur at levels different for each individual patient, and in accordance with Society for Cardiovascular Angiography & Interventions guidelines.
- Limit contrast. Pay attention to how much contrast has been administered and aim to use the least amount possible to obtain necessary images.
- Observe patient labs. If a patient exhibits a risk factor and was administered contrast, observe their lab values closelyto make sure they don’t have an increase in creatinine from baseline or greater than 0.3 mg/dl.
VASCULAR COMPLICATIONS AND HEMOSTATIS
Because catheterization lab procedures involve vascular access, vascular complications are always a concern. The following should be areas of focus:
- Assess risk. Determine in advance of procedures: What is the chance that this patient will experience vascular complications such as bleeding, hematoma, dissection, and aneurysm?
- Determine the access point: Radial access has been shown to decrease bleeding, the chance of vascular complications, and mortality in patients with stents. Today it is the default. However, femoral access is still sometimes the chosen approach. When this is the case, make sure femoral access is ultrasound guided. Seven randomized controlled trial studies comparing ultrasound guided access to standard practice revealed that ultrasound-guided access for femoral sites increased success in first attempts, reduced time to access, and led to fewer vascular complications and hematomas. A few more access considerations:
- Consider the sheath. The larger the sheath, the bigger the hole, therefore increasing risk.
- Anticoagulation or dual antiplatelet therapy. Patients on either of these treatments have increased risk of vascular complication.
- Achieve hemostasis. Manual compression, mechanical clamps, and arterial puncture closing devices are options for achieving and sustaining hemostasis, or cessation of bleeding. Regardless of method(s) used, it’s critical to perform frequent assessments, educate the patient (“Keep this leg straight,” for example, or “You can’t lift anything with this hand.”), and communicate clearly to subsequent caregivers. Ensure they know the access location, whether and which device was used for hemostasis, any complications, and other information integral to their ability to provide care.
SEDATION & MEDICATION SAFETY
Most patients undergoing procedures in the cardiac catheterization will receive moderate sedation; however, some will require general anesthesia. Anesthesia type is influenced by patient acuity, case specifics, patient medical history, and other factors, with the unfaltering goal of a depressed level of consciousness that allows a patient maintain oxygenation, ventilation, and airway control independently while receiving comfort.
Whichever sedation is administered, American Society of Anesthesiologists guidelines mandate documentation on two fronts: documentation of a patient’s suitability to receive said sedation and the patient’s Mallampati score, or the size of the tongue base in relation to the oropharyngeal opening to gauge airway viability.[4] Both require commensurate assessments related to airway protection.
Typically, sedation involves a combination of benzodiazepines and opioids, but caution needs to be exercised in administering benzodiazepines to certain patients, including the elderly patient population. Remember, too, that opiates sometimes are not needed. Whatever the specifics, it’s critical that nurses know their board of nursing (BON) regulations, which are state-determined mandates for what nurses can do in relation to sedation. Above all, make sure to double-check high-alert medications. Cardiac catheterization lab teams employ and manage several high-alert medications, including heparin. Double-check your work at every point along the way and know your basic rights when it comes to sedation (and larger medication) administration.
EMERGENCY RESPONSE
Patients can experience emergencies in the catheterization lab. Appropriate monitoring and prevention as well as an emergency response plan understood by all team members are essential.
In terms of prevention, all patients (even those undergoing elective procedures) need to have non-invasive hemodynamic monitoring as well as SpO2 monitoring. If patients come in with a STEMI or are otherwise deemed high risk, defibrillator pads (or electrodes) should be placed on their body in case they go into lethal arrhythmia. Also make sure to have a patent IV prior to the procedure to ensure immediate IV access in the event of an emergency.
In terms of emergency preparedness: In advance of the procedure, everyone involved needs to determine how they will individually and collectively manage and respond in the event of any of the following. Preparation should include a clear plan for how the emergency response team will be called as well as confirmation that all related equipment is available and readily accessible:
- Arrhythmias
- Hypotension
- Allergic reactions
- Access site complications
ENVIRONMENTAL AND EQUIPMENT SAFETY
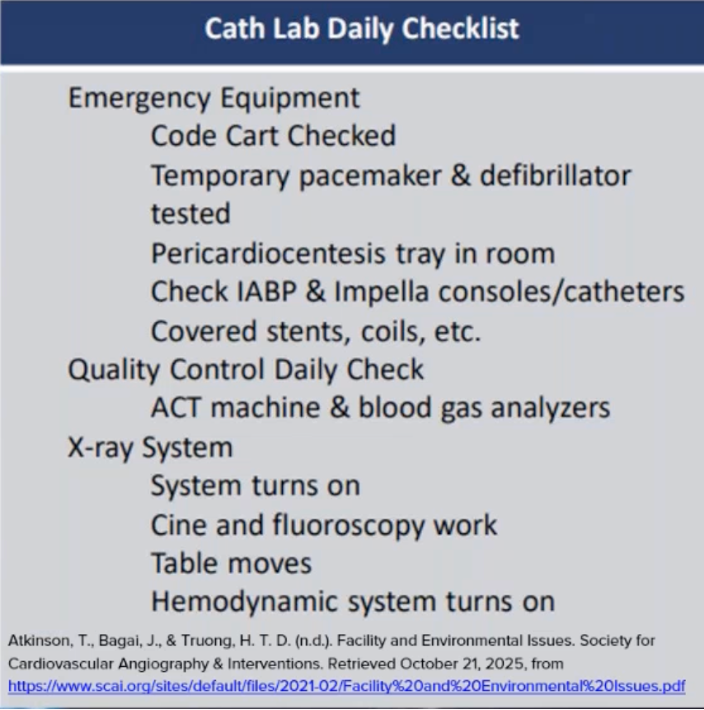
Catheterization labs are sterile environments. Environmental and equipment safety, including infection control, is key. The general recommendation is that labs should be deep cleaned once a day but also spot cleaned between each procedure and as needed if extremely soiled. Doors need to be closed when not in use and during all procedures and documentation of relative humidity as well as temperature (part of regulatory compliance) needs to be kept up to date. It’s furthermore important to ensure that all equipment and devices are in service and have not yet expired.
Here is a catheterization lab checklist featuring additional environmental and equipment-related tasks to be completed daily:
POST-PROCEDURAL SAFETY CHECKS
Lastly, be sure to incorporate post-procedural safety checks into protocol for every catheterization lab procedure. Post-procedural checklists are important for many reasons including this one: They arm the person receiving a patient – whether an ICU nurse, family and friends, home care, or the patient him/herself – with the information necessary for ongoing care.
It is imperative to share and discuss the procedure’s findings, complications when applicable, and any additional interventions that were performed. If the patient received sedation, how much and what type? Were additional medications given, including heparin, Plavix, and/or aspirin? Review general vital signs and intracardiac and hemodynamic values.
Hemostasis should also be elaborated upon: Was it radial? Femoral? Venous? How was homeostasis maintained or achieved? Is there anything else that should be highlighted, such as bedrest time? In outpatient settings, make sure that the patient (and care teams, when applicable) is aware of follow-up care, which can consist of the following:
- Labs and imaging
- Medication reconciliation
- Activity restrictions
- Follow-up appointments
In inpatient settings (if a patient is moving from the catheterization lab to critical care or some other inpatient setting, for example) make sure the receiving professionals receiving them know:
- Patient pulse and vital signs
- Procedure site
Eager to learn more about the precess of establishing a collaborative culture of safety in your medical setting? Earn one free contact hour by listening to the full on-demand webinar.
Sarah Vance, MSN, RN, CCRN

With over 15 years of critical care experience, Sarah is dedicated to educating and mentoring nurses, both new and new to critical care. Sarah has a knack for simplifying complex concepts and bringing a lighthearted approach to the often intense ICU environment.
She shares valuable free open-access medical education content on social media, covering topics such as intra-aortic balloon pump placement, sedation and pain management for ventilated patients, and safe blood transfusion administration, all crucial for critical care nurses. She sees the nurse holistically, recognizing the emotional and interpersonal aspects in addition to the technical skills and protocols. She understands that nursing involves the heart, emotions, relationships, communication, and ongoing self-reflection.
[1] https://www.collaborative-safety.com/