The Evolution of Pressure Injuries

Pressure injuries are complex, clinically and historically. Discover how modern pressure injury terminology came to pass and brush up on current staging recommendations and prevention strategies. Listen to the full on-demand webinar to earn one contact hour.
It’s tempting to consider pressure injuries a 21st century problem, tied to modern healthcare. This is due at least in part to the prevalence of pressure injuries among acute care patients, related medical claims, and high financial stakes across it all. In the United States, the estimated cost of care for a pressure injury Stage 3 or higher is anywhere from $21,000 to $151,000 per pressure injury. Pressure injuries are the number one malpractice claim in the nation, with some cases settling for upward of a million dollars.
In reality, pressure injuries pre-date modern medicine by millennia. Pressure injuries were found on Egyptian mummies dating back five thousand years, to 2500 BC. In 460 BC, Hippocrates described a person believed to be suffering from pressure injuries. And in his Renaissance-era autobiography, Ambroise Paré, a French Army barber-surgeon and the founding father of med-surg, described a pressure ulcer developing on a wounded soldier.
Yet while the existence of pressure injuries across time is undisputed, causation and related nomenclature has been less straightforward. In 1877, French neurologist[1] Jean-Martin Charcot laid forth his neuropathic theory – the belief that central nervous system damage, rather than pressure, is responsible for pressure injuries (which he called decubitus ulcers). This theory was subsequently challenged by Charles-Édouard Brown-Sequard[2] who observed that, in guinea pigs, pressure injuries did not develop in the absence of pressure (and existing pressure injuries healed). However, time has shown Brown-Sequard’s conclusion to be less than sound, as we’ll elaborate on below.
In short, debate surrounding pressure injury causation continues to this day, as do efforts to unify pressure injury-related terminology. This is largely a reflection of pressure injuries’ multi-faceted clinical past.
WHAT’S IN A NAME?
Bedsores. Pressure wounds. Ulcers. Many names and phrases have been used over the years, formally and informally, to describe what are now clinically defined as pressure injuries.
So how did we get from decubitus ulcer in 1800s (a term still used in Medicare-related regulation relative to pressure injuries, astoundingly) to pressure injury?
A quick primer:
In 1975, J. Darrell Shea[3] created a system for classifying pressure sores. In the late 1980s, that system evolved to become the four-category system we know today, except it used the term pressure ulcer.
From an accuracy standpoint, however, both sore and ulcer proved insufficient in describing these skin events. Beyond the inherent problems of incorrect naming, this disconnect also had negative repercussions for ICD-10 coding necessary for medical billing.
In 2007, the National Pressure Ulcer Advisory Panel categorized unstageable and suspected deep tissue injuries as types of pressure ulcers. Then, in 2016, the National Pressure Ulcer Advisory Panel rebranded as the National Pressure Injury Advisory Panel (NPIAP), solidifying pressure injury as agreed-upon industry-wide nomenclature. Injury, after all, can encompass a wide range of skin issues. It’s also broad enough to include lesions, such as intact skin injuries, or deep tissue pressure injuries.
Under the pressure injury umbrella, acute forms of pressure injuries are categorized as wounds. Meanwhile, chronic forms are characterized as ulcers. While wounds are always caused by an external force, ulcers stem from internal causation.
A BRIEF STAGING REVIEW
Pressure injury prevention and treatment depends on a clear understanding of each defined pressure injury stage. It is worthwhile for healthcare professionals to brush up from time to time on demarcation between these. Four numerical categories exist for pressure injuries; however, pressure injuries can ultimately fall into one of six total categories:
Pressure Injury Stage 1
- Intact skin with non-blanchable redness of a localized area, Stage 1 pressure injuries typically present overtop of a bony prominence.
- Keep in mind: Darkly pigmented skin might not have visible blanching. Its color may differ from the surrounding area.
- Visual observation is not enough. Providers must touch skin to determine whether or not blanching is present.
Pressure Injury Stage 2
- Partial thickness loss of dermis presenting as a shallow open ulcer with a red-pink wound bed, without slough.
- May also present as an intact or open/ruptured serum-filled blister.
- Presents as a shiny or dry shallow ulcer without bruising or, again, slough.
- Note: Stage 2 should not be used to describe skin tears, tape burns, perineal dermatitis, maceration, or excoriation.
Pressure Injury Stage 3
- Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or muscle are not exposed.
- Slough may be present but not to the extent that it obscures the depth of tissue loss. May include slough undermining and/or tunneling.
- Contrary to common belief, measurable depth cannot be used to characterize Stage 3 pressure injuries, as depth and related severity vary by anatomical location. Take a human cheek, for example. A pressure injury considered deep on the cheek would be comparatively shallow on the buttock.
Pressure Injury Stage 4
- The last of the numerical stages, Stage 4 is characterized by full thickness tissue loss with exposed bone, tendon, or muscle.
- Can also expose ligaments, joint capsules, or hardware.
- Slough or eschar may be present on some parts of the wound bed. Slough often features undermining and/or tunneling.
Unstageable Pressure Injury
- Unstageable pressure injuries are those whose stage can’t be readily determined[4].
- Generally characterized by full-thickness tissue loss in which the ulcer base is covered by non-viable tissue such as slough (yellow, tan, gray, green, and/or brown) or eschar (tan, brown, and/or black) in the wound bed.
- Non-viable tissue can sometimes have leathery or tough textures.
- Eschar can be stable or unstable.
- Stable eschar is a dry wound with no lifting of the wound edge, no erythema, and no exudate coming out from underneath.
- In unstable eschar, edges are lifting. There can be signs of inflammation or infection, such as purulent drainage or seropurulent drainage coming from the edges
- Potentially malodorous.
DEEP TISSUE PRESSURE INJURIES
- Bottom-up soft tissue damage that works its way from the bone area to the skin.
- Initially presents as an intact epithelium – typically a purple or maroon localized area of discolored intact skin or blood-filled blister.
- Area may be preceded by tissue that is painful, firm, mushy, boggy, warmer, or cooler compared to adjacent tissue.
- Rapidly deteriorates.
- It can be helpful to think of a deep tissue pressure injury as a heart attack of the skin – a anoxic injury to the skin and soft tissue that progresses to sloughing of some superficial tissue, followed by necrosis and full thickness tissue loss.
PRESSURE INJURIES: PREVENTABLE?
As touched on above, questions of how and whether pressure injuries are preventable continue to evolve. Historically considered a reflection of insufficient care, stances on pressure injuries started shifting in 2014, when Edsberg and Langemo et al. published groundbreaking research concluding that, in light of clinical complexities and the constellation of comorbidities encountered in today’s healthcare environment, it is reasonable to state that not all pressure injuries are avoidable or preventable. The skin, after all, is the largest organ of the body; its integrity is impacted by elements outside of caregiver control including age, medications, microclimate, optimal functioning of other organs, and concomitant diseases and illnesses.
The National Pressure Injury Advisory Panel today defines an unavoidable pressure injury as one that develops even when the provider has:
- Evaluated the individual’s clinical condition and pressure injury risk factors.
- Defined and implemented interventions that were consistent with individual needs, goals, and recognized standards of practice.
- Monitored and evaluated the impact of the interventions.
- Revised the approaches as appropriate.
Put another way, while progress has been made healthcare-wide in reducing the incidence of pressure injuries, and while some injuries can be acutely prevented, an incidence of zero may not be attainable. Conversations around this topic are ongoing, and increasingly include discussion of skin failure.
*For information related to the prevention and management of pressure injuries refer to the NPIAP website.
SKIN FAILURE DEFINED
The NPIAP and the Post-Acute Wound & Skin Integrity Council are two organizations working diligently to define skin failure, assigning corresponding ICD-10 codes, and clarifying the relationship between skin failure and pressure injuries.
Skin failure is defined as an event in which skin and underlying tissue die due to hypoperfusion that occurs concurrently with severe dysfunction or failure of other organ systems. It is seen most often in patients who are hemodynamically unstable.
The latest research organizes skin failure into three categories: Acute, chronic, and end-of-life.
Acute skin failure is hypoperfusion of the skin that results in tissue death in the setting of critical illness.
Chronic skin failure, meanwhile, is associated with a gradual deterioration of skin integrity due to chronic diseases and the effects of aging. There is a steady decline in the condition of skin and underlying tissue, typically stemming from a variety of health issues rather than an immediate trauma, such as with a critical illness.
Lastly, end-stage skin failure is a critical condition in which the skin can no longer effectively perform its essential functions due to severe damage, disease, or deterioration. This stage can be characterized by symptoms such as extensive wounds, ulcers, or lesions, lack of skin integrity, constant pain, or increased susceptibility to infections.
Risk factors for all three types of skin failure include:
- Acute and chronic conditions
- Age-related changes
- Structural impairment
- Pharmacologic factors
- The dying process
- Miscellaneous and dermatological conditions, such as Stevens-Johnson syndrome (SJS).
From a pathophysiology standpoint, the following can also contribute to skin failure:
- Hypoperfusion
- Hypoxia
- Inflammation
- Inflammation-induced vascular permeability
- Inflammation-induced edema
Finally, all variety of barrier disruptions can also increase susceptibility to skin failure:
- Physical
- Chemical
- Immunological
- Microbiome disruption
SPOTLIGHT ON END-OF-LIFE SKIN FAILURE
When a patient has a pressure injury, caregivers can come under scrutiny. However, increasing evidence points to unique and unpreventable physiological events that can occur during, and as part of, the dying process.
In the medical community, skin-related manifestations of such events are summarized as SCALE, an acronym for Skin Changes at Life’s End. SCALE affects skin and soft tissue. They can manifest as observable changes in skin color, turgor, or integrity, or as a subjective symptom like pain. SCALE highlights the fact that not all skin changes are necessarily caused by pressure; often at life’s end they are caused by larger vascular compromise.
Kennedy terminal ulcers, often abbreviated KTU, are the most readily defined example. Kennedy terminal ulcers are named in honor of Dr. Patricia Kennedy, a renowned physician and wound care pioneer who first identified and researched them, and contributed to management strategies. This unique type of pressure ulcer presents in some, but not all, individuals nearing end of life. Marked by sudden onset and rapid progression, KTUs are known to be shaped like a pear, butterfly, or horseshoe, and are typically red, yellow, or purple. When they appear, death is imminent.
HAPI IN CRITICAL CARE AND RELATED MITIGATION
It’s no secret that there are high instances of pressure injuries in acute care settings. Ten to 20 percent of critical care unit patients will develop a pressure injury.
When they develop in a clinical setting, pressure injuries become known as hospital-acquired pressure injuries, or HAPIs. Critical care patients in particular are at increased risk of HAPIs for a multitude of possible reasons:
- Length of stay, which is typically longer than non-critical patients
- Immobility
- Comorbidities
- Poor oxygenation or perfusion
- Hemodynamic instability
- Medical devices, placement of which can contribute to pressure and therefore pressure injuries
- Low neurological functioning/delirium
- Actively dying
- Vasopressors
Of these, vasopressors are often overlooked, but shouldn’t be. Patients treated with vasopressors are 4.8 times more likely to develop a pressure injury.
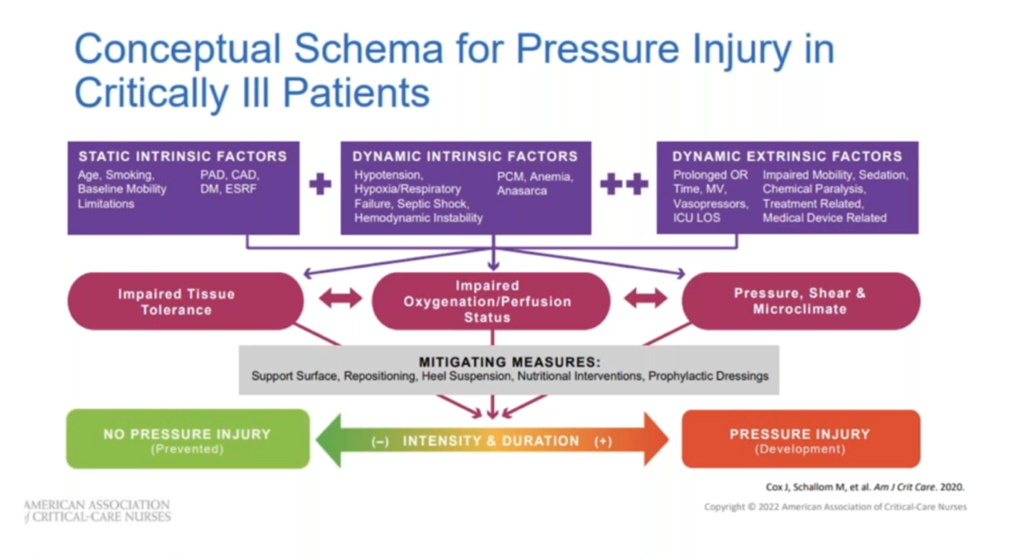
In 2020, Jill Cox developed a conceptual schema for pressure injury development in critically ill patients; it was published in the American Journal of Critical Care the same year. This schema features static intrinsic factors, dynamic intrinsic factors, and dynamic extrinsic factors, showing how these can combine with additional clinical circumstances to elevate the likelihood of, or directly lead to, pressure injury:
PRESSURE INJURY PREVENTION AND TREATMENT
A systematic approach to prevention injury risk assessment is one of the best steps healthcare settings can take to prevent and treat injuries. Systematic in this context means standardized, high-frequency processes for identifying at-risk patients. In acute care, The Braden Scale for Predicting Pressure Sore Risk and the Braden QD scales are common tools. However, they can only be successful if supported by an institutional commitment to proactive pressure injury prevention.
Successful prevention and treatment also hinge on the implementation of individualized care plans that include regular repositioning, skincare, nutritional support, and support services, as well as other essential components of care:
- Heel offloading
- Moisture control
- Toilet scheduling
- Regular risk assessments
- Minimized friction and shearing forces
- Hydration
- Barriers
- Prophylactic dressings
Careful and accurate documentation can also go a long way toward preventing and treating pressure injuries, in part because patient non-adherence is among the often-overlooked contributors. Notes on non-adherence should always include exact statements made by a patient, the education you provided, and the patient’s response.
It is also important to alter a patient’s treatment plan based upon a patient’s response and subsequent education provided. When a patient is educated and making their own decisions, liability risk decreases. Even more, the patient has a higher likelihood of adherence.
In conclusion, the fact that skin is an organ contributes to complexity surrounding pressure injury history, wound terminology, and treatment, but can also shed light on the more tough-to-pinpoint aspects of pressure injury prevention, staging, and care.
Want to delve deeper into the clinical and historical evolution of pressure injuries? Learn more and earn one free contact hour by listening to the full on-demand webinar.
[3] https://pubmed.ncbi.nlm.nih.gov/30720473/